

Cost-effectiveness of fracture prevention in men who receive androgen deprivation therapy for localized prostate cancer
- PMID: 20479027
- PMCID: PMC5468170
- DOI: 10.7326/0003-4819-152-10-201005180-00002
Cost-effectiveness of fracture prevention in men who receive androgen deprivation therapy for localized prostate cancer
Abstract
Background: Androgen deprivation therapy (ADT) increases the risk for fractures in patients with prostate cancer.
Objective: To assess the cost-effectiveness of measuring bone mineral density (BMD) before initiating ADT followed by alendronate therapy in men with localized prostate cancer.
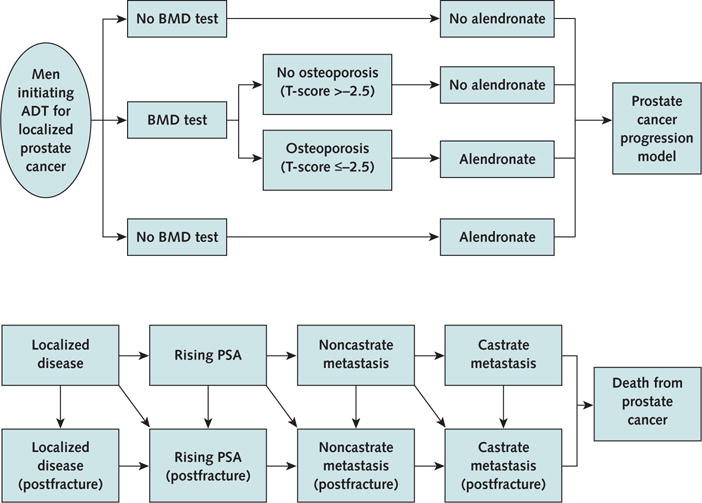
Design: Markov state-transition model simulating the progression of prostate cancer and the incidence of hip fracture.
Data sources: Published literature.
Target population: A hypothetical cohort of men aged 70 years with locally advanced or high-risk localized prostate cancer starting a 2-year course of ADT after radiation therapy.
Time horizon: Lifetime.
Perspective: Societal.
Intervention: No BMD test or alendronate therapy, a BMD test followed by selective alendronate therapy for patients with osteoporosis, or universal alendronate therapy without a BMD test.
Outcome measures: Incremental cost-effectiveness ratio (ICER), measured by cost per quality-adjusted life-year (QALY) gained.
Results of base-case analysis: The ICERs for the strategy of a BMD test and selective alendronate therapy for patients with osteoporosis and universal alendronate therapy without a BMD test were $66,800 per QALY gained and $178,700 per QALY gained, respectively.
Results of sensitivity analyses: The ICER for universal alendronate therapy without a BMD test decreased to $100,000 per QALY gained, assuming older age, a history of fractures, lower mean BMD before ADT, or a lower cost of alendronate.
Limitations: No evidence shows that alendronate reduces actual fracture rates in patients with prostate cancer who receive ADT. The model predicted fracture rates by using data on the surrogate BMD end point.
Conclusion: In patients starting adjuvant ADT for locally advanced or high-risk localized prostate cancer, a BMD test followed by selective alendronate for those with osteoporosis is a cost-effective use of resources. Routine use of alendronate without a BMD test is justifiable in patients at higher risk for hip fractures.
Conflict of interest statement
Figures
Comment in
-
Prostate cancer: Is fracture prevention therapy cost-effective in patients with prostate cancer treated with ADT?Nat Rev Urol. 2010 Jul;7(7):363. doi: 10.1038/nrurol.2010.90. Nat Rev Urol. 2010. PMID: 20665935 No abstract available.
-
Socioeconomic factors, urological epidemiology and practice patterns.J Urol. 2010 Nov;184(5):1991-4. doi: 10.1016/j.juro.2010.07.024. Epub 2010 Sep 19. J Urol. 2010. PMID: 22520001 No abstract available.
References
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Prostate Cancer. Fort Washington, PA: National Comprehensive Cancer Network; 2010. v.l.2010. Accessed at www.nccn.org/professionals/physician_gls/PDF/prostate.pdf [registration required] on 1 February 2010. - PubMed
-
- American Urological Association. Guideline for the management of clinically localized prostate cancer: 2007 Update. Baltimore: American Urological Assoc; 2007. Accessed at www.auanet.org/content/guidelines-and-quality-care/clinical-guidelines/m... on 1 February 2010.
-
- Wilt TJ, MacDonald R, Rutks I, Shamliyan TA, Taylor BC, Kane RL. Systematic review: comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann Intern Med. 2008;148:435–48. - PubMed
-
- Maillefert JF, Sibilia J, Michel F, Saussine C, Javier RM, Tavernier C. Bone mineral density in men treated with synthetic gonadotropin-releasing hormone agonists for prostatic carcinoma. J Urol. 1999;161:1219–22. - PubMed
-
- Daniell HW, Dunn SR, Ferguson DW, Lomas G, Niazi Z, Stratte PT. Progressive osteoporosis during androgen deprivation therapy for prostate cancer. J Urol. 2000;163:181–6. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials