

A cluster-randomized trial to improve stroke care in hospitals
- PMID: 20479363
- PMCID: PMC2875128
- DOI: 10.1212/WNL.0b013e3181df096b
A cluster-randomized trial to improve stroke care in hospitals
Abstract
Objective: We evaluated the effect of performance feedback on acute ischemic stroke care quality in Minnesota hospitals.
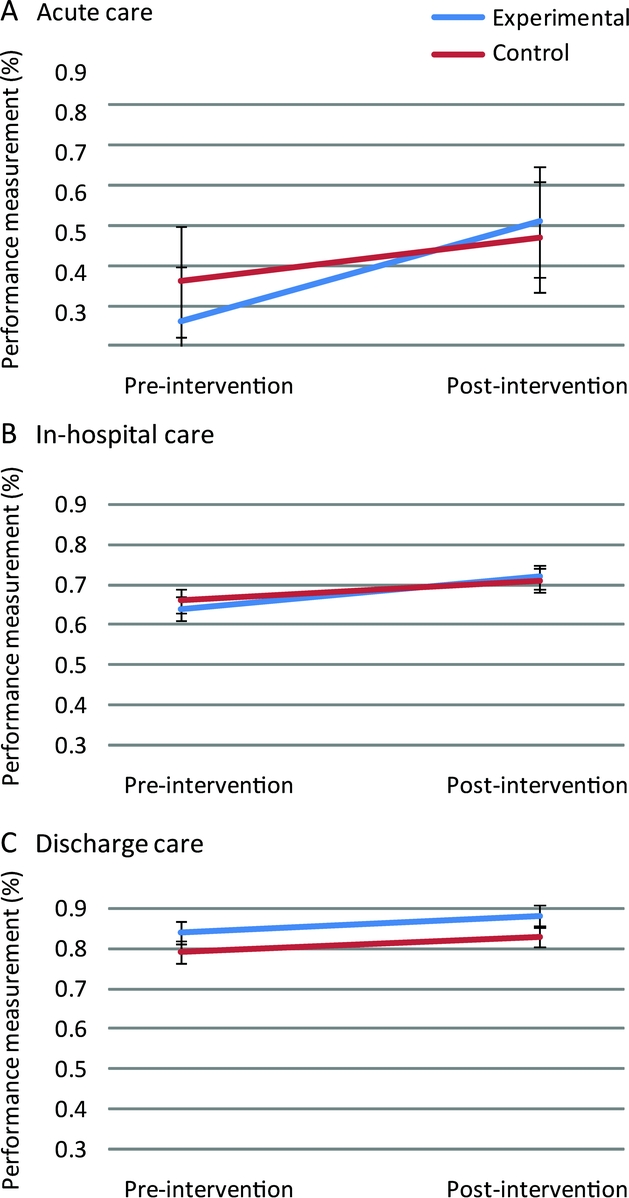
Methods: A cluster-randomized controlled trial design with hospital as the unit of randomization was used. Care quality was defined as adherence to 10 performance measures grouped into acute, in-hospital, and discharge care. Following preintervention data collection, all hospitals received a report on baseline care quality. Additionally, in experimental hospitals, clinical opinion leaders delivered customized feedback to care providers and study personnel worked with hospital administrators to implement changes targeting identified barriers to stroke care. Multilevel models examined experimental vs control, preintervention and postintervention performance changes and secular trends in performance.
Results: Nineteen hospitals were randomized with a total of 1,211 acute ischemic stroke cases preintervention and 1,094 cases postintervention. Secular trends were significant with improvement in both experimental and control hospitals for acute (odds ratio = 2.7, p = 0.007) and in-hospital (odds ratio = 1.5, p < 0.0001) care but not discharge care. There was no significant intervention effect for acute, in-hospital, or discharge care.
Conclusion: There was no definite intervention effect: both experimental and control hospitals showed significant secular trends with performance improvement. Our results illustrate the potential fallacy of using historical controls for evaluating quality improvement interventions.
Classification of evidence: This study provides Class II evidence that informing hospital leaders of compliance with ischemic stroke quality indicators followed by a structured quality improvement intervention did not significantly improve compliance more than informing hospital leaders of compliance with stroke quality indicators without a quality improvement intervention.
Figures

References
-
- Kleindorfer D, Lindsell CJ, Brass L, Koroshetz W, Broderick JP. National US estimates of recombinant tissue plasminogen activator use: ICD-9 codes substantially underestimate. Stroke 2008;39:924–928. - PubMed
-
- Holloway RG, Benesch C, Rush SR. Stroke prevention: narrowing the evidence-practice gap. Neurology 2000;54:1899–1906. - PubMed
-
- Holloway RG, Vickrey BG, Benesch C, Hinchey JA, Bieber J, National Expert Stroke Panel. Development of performance measures for acute ischemic stroke. Stroke 2001;32:2058–2074. - PubMed
-
- Kernan WN, Viscoli CM, Brass LM, Makuch RW, Sarrel PM, Horwitz RI. Blood pressure exceeding national guidelines among women after stroke. Stroke 2000;31:415–419. - PubMed
-
- Reeves MJ, Arora S, Broderick JP, et al. Acute stroke care in the US: Results from 4 pilot prototypes of the Paul Coverdell National Acute Stroke Registry. Stroke 2005;36:1232–1240. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials