

Site and timing of first relapse in stage III melanoma patients: implications for follow-up guidelines
- PMID: 20479405
- PMCID: PMC3664035
- DOI: 10.1200/JCO.2009.26.2063
Site and timing of first relapse in stage III melanoma patients: implications for follow-up guidelines
Abstract
Purpose: Stage III melanoma is associated with a high risk of relapse and mortality. Nevertheless, follow-up guidelines have largely been empirical rather than evidence-based.
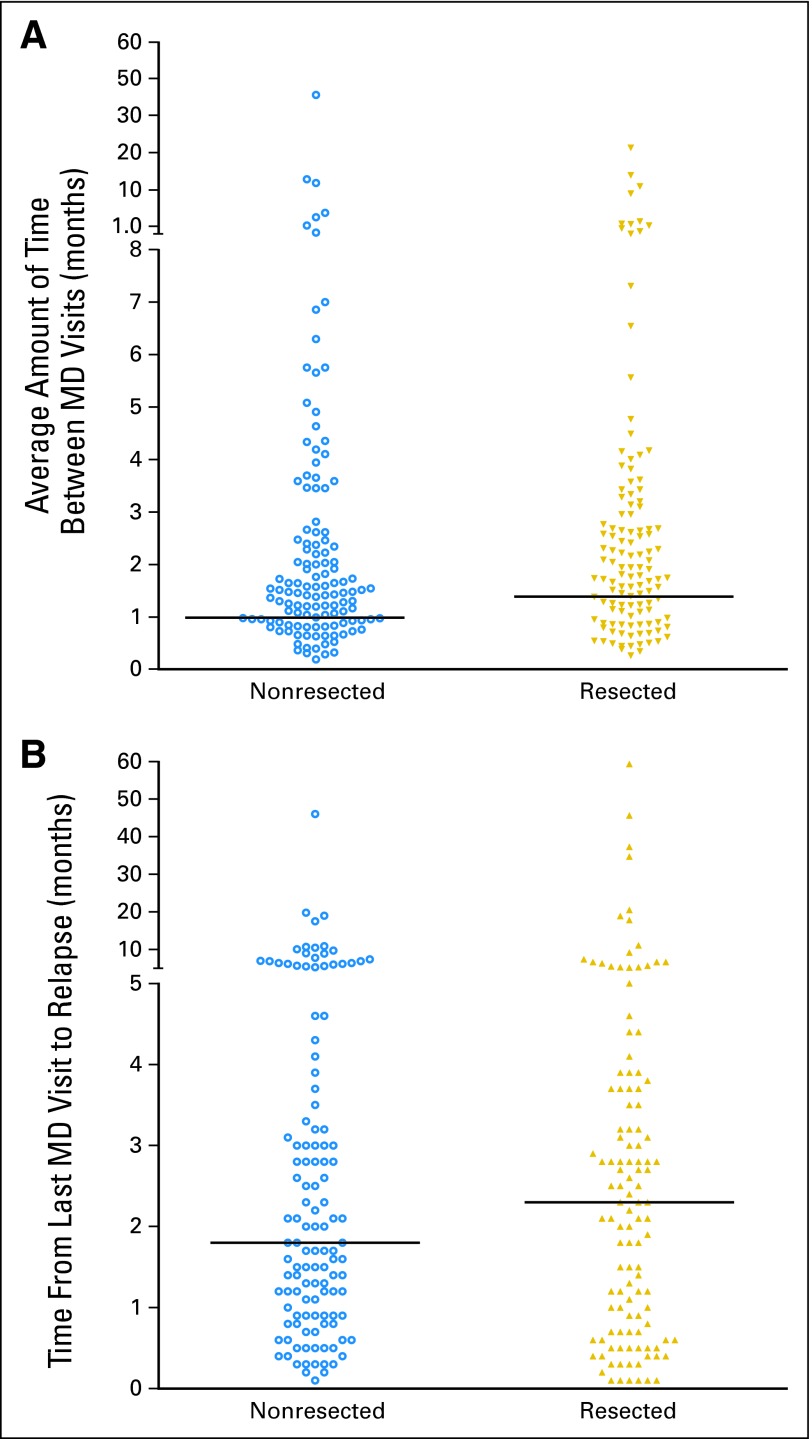
Patients and methods: Clinical records of stage III patients with no evidence of disease seen at Memorial Sloan-Kettering Cancer Center (MSKCC) between 1992 and 2004, who ultimately relapsed, were reviewed retrospectively to evaluate date of first relapse, time to first relapse, method of first relapse detection, and survival. We also determined overall 5-year relapse-free survival (RFS) of all stage III patients seen at MSKCC during this period.
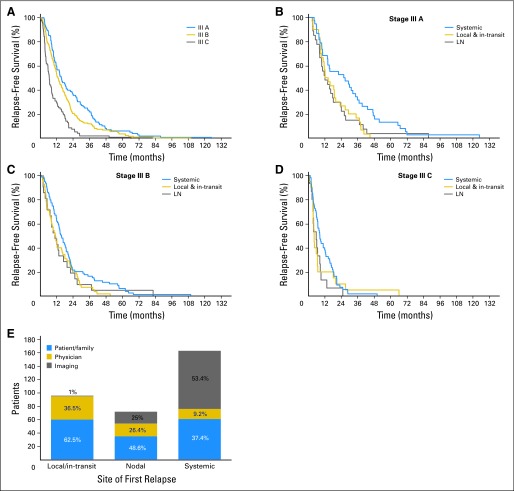
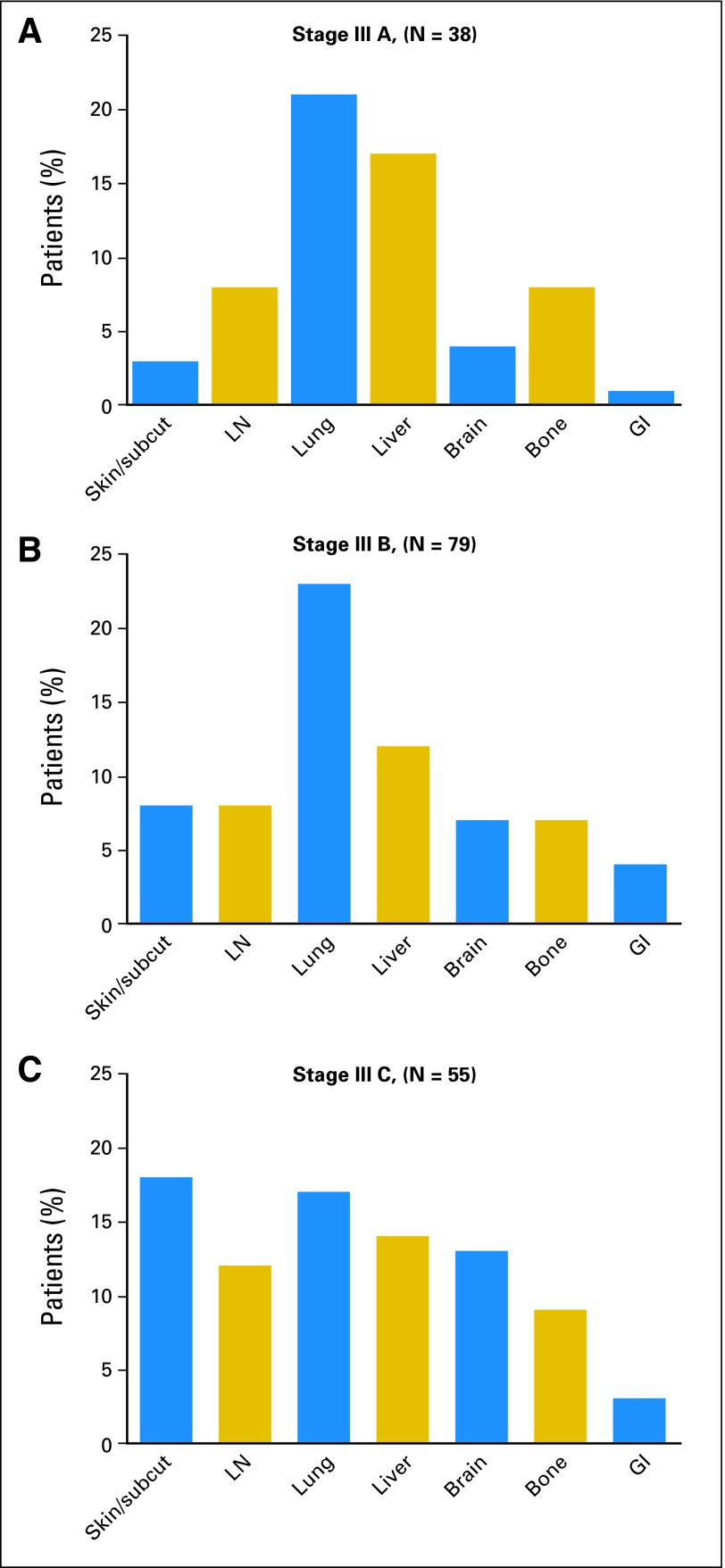
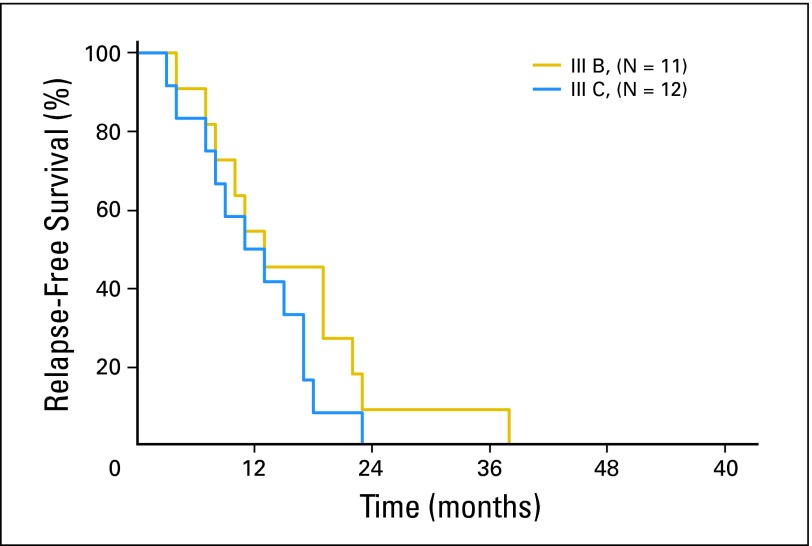
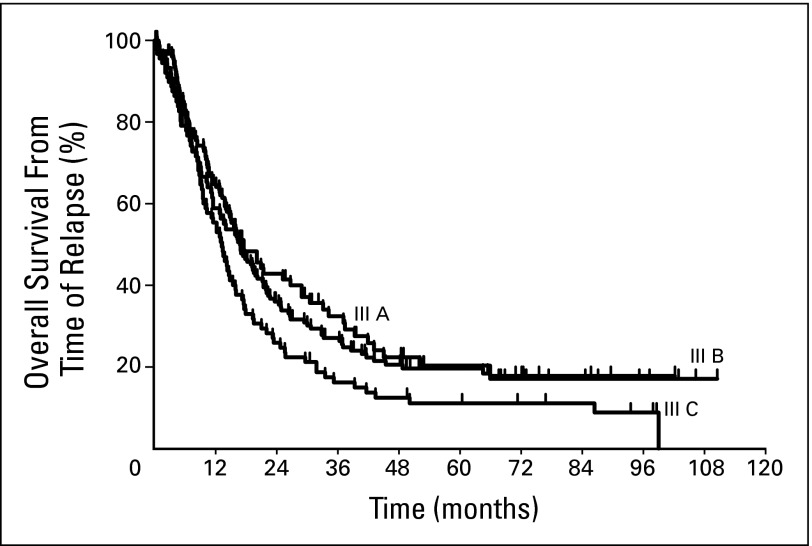
Results: The overall 5-year RFS for stage IIIA, IIIB, and IIIIC patients was 63%, 32%, and 11%, respectively. Among relapsing patients, 340 had adequate follow-up to be evaluable for all parameters. Site of first relapse was local/in-transit (28%), regional nodal (21%), or systemic (51%). First relapses were detected by the patient or family, physician, or by screening radiologic tests in 47%, 21%, and 32% of patients, respectively. Multivariate analysis revealed that better overall survival was associated with younger age and first relapse being local/in-transit or nodal, asymptomatic, or resectable. For each substage, we estimated site-specific risk of first relapse.
Conclusion: Patients detected almost half of first relapses. Our data suggest that routine physical examinations beyond 3 years for stage IIIA, 2 years for stage IIIB, and 1 year for stage IIIC patients and radiologic imaging beyond 3 years for stages IIIA and IIIB and 2 years for stage IIIC patients would be expected to detect few first systemic relapses.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Balch CM, Buzaid AC, Soong SJ, et al. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J Clin Oncol. 2001;19:3635–3648. - PubMed
-
- Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic factors analysis of 17,600 melanoma patients: Validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol. 2001;19:3622–3634. - PubMed
-
- Garbe C, Paul A, Kohler-Spath H, et al. Prospective evaluation of a follow-up schedule in cutaneous melanoma patients: Recommendations for an effective follow-up strategy. J Clin Oncol. 2003;21:520–529. - PubMed
-
- Poo-Hwu WJ, Ariyan S, Lamb L, et al. Follow-up recommendations for patients with American Joint Committee on Cancer Stages I-III malignant melanoma. Cancer. 1999;86:2252–2258. - PubMed
-
- Francken AB, Shaw HM, Accortt NA, et al. Detection of first relapse in cutaneous melanoma patients: Implications for the formulation of evidence-based follow-up guidelines. Ann Surg Oncol. 2007;14:1924–1933. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
