

Retropubic versus transobturator midurethral slings for stress incontinence
- PMID: 20479459
- PMCID: PMC2962585
- DOI: 10.1056/NEJMoa0912658
Retropubic versus transobturator midurethral slings for stress incontinence
Abstract
Background: Midurethral slings are increasingly used for the treatment of stress incontinence, but there are limited data comparing types of slings and associated complications.
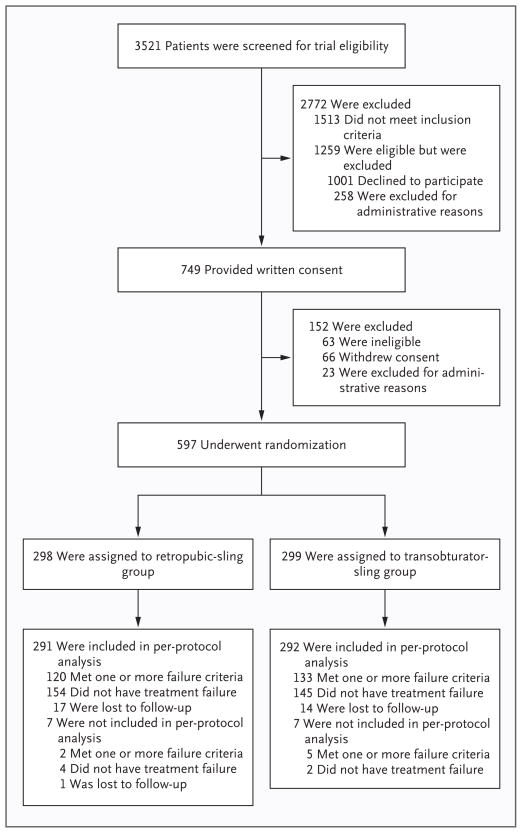
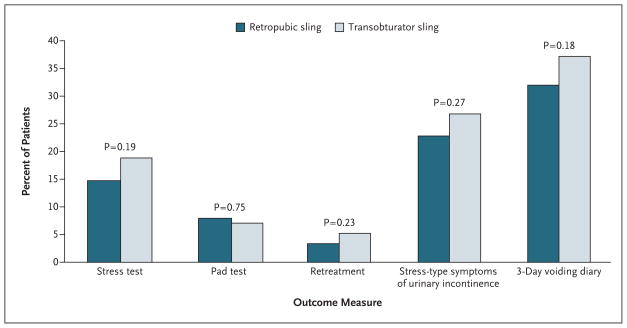
Methods: We performed a multicenter, randomized equivalence trial comparing outcomes with retropubic and transobturator midurethral slings in women with stress incontinence. The primary outcome was treatment success at 12 months according to both objective criteria (a negative stress test, a negative pad test, and no retreatment) and subjective criteria (self-reported absence of symptoms, no leakage episodes recorded, and no retreatment). The predetermined equivalence margin was +/-12 percentage points.
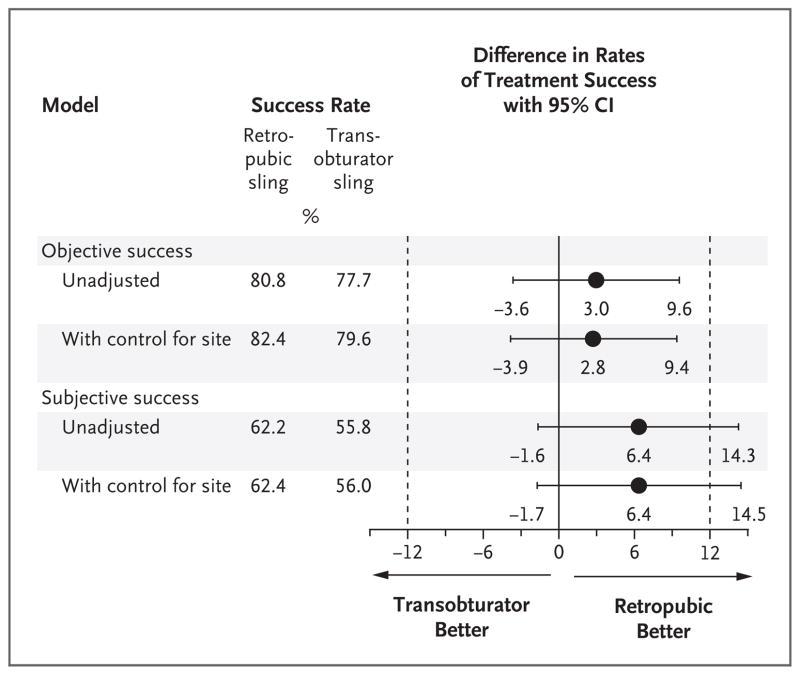
Results: A total of 597 women were randomly assigned to a study group; 565 (94.6%) completed the 12-month assessment. The rates of objectively assessed treatment success were 80.8% in the retropubic-sling group and 77.7% in the transobturator-sling group (3.0 percentage-point difference; 95% confidence interval [CI], -3.6 to 9.6). The rates of subjectively assessed success were 62.2% and 55.8%, respectively (6.4 percentage-point difference; 95% CI, -1.6 to 14.3). The rates of voiding dysfunction requiring surgery were 2.7% in those who received retropubic slings and 0% in those who received transobturator slings (P=0.004), and the respective rates of neurologic symptoms were 4.0% and 9.4% (P=0.01). There were no significant differences between groups in postoperative urge incontinence, satisfaction with the results of the procedure, or quality of life.
Conclusions: The 12-month rates of objectively assessed success of treatment for stress incontinence with the retropubic and transobturator approaches met the prespecified criteria for equivalence; the rates of subjectively assessed success were similar between groups but did not meet the criteria for equivalence. Differences in the complications associated with the two procedures should be discussed with patients who are considering surgical treatment for incontinence. (ClinicalTrials.gov number, NCT00325039.)
2010 Massachusetts Medical Society
Figures
Comment in
-
What's best in the treatment of stress urinary incontinence?N Engl J Med. 2010 Jun 3;362(22):2124-5. doi: 10.1056/NEJMe1005367. Epub 2010 May 17. N Engl J Med. 2010. PMID: 20479458 No abstract available.
-
Need for standardization in definition of success in clinical trials on stress urinary incontinence.Curr Urol Rep. 2010 Nov;11(6):361-3. doi: 10.1007/s11934-010-0138-0. Curr Urol Rep. 2010. PMID: 20821357 No abstract available.
-
Re: Retropubic versus transobturator midurethral slings for stress incontinence.J Urol. 2012 Jan;187(1):202-4. doi: 10.1016/j.juro.2011.09.139. Epub 2011 Nov 25. J Urol. 2012. PMID: 22153438 No abstract available.
-
Re: Baseline urodynamic predictors of treatment failure 1 year after mid urethral sling surgery: C. W. Nager, L. Sirls, H. J. Litman, H. Richter, I. Nygaard, T. Chai, S. Kraus, H. Zyczynski, K. Kenton, L. Huang, J. Kusek and G. Lemack for the urinary incontinence treatment network J Urol 2011; 186: 597-603.J Urol. 2012 Jun;187(6):2282-3; author reply 2283-4. doi: 10.1016/j.juro.2012.01.131. Epub 2012 Apr 13. J Urol. 2012. PMID: 22503045 No abstract available.
References
-
- Melville JL, Katon W, Delaney K, Newton K. Urinary incontinence in US women: a population-based study. Arch Intern Med. 2005;165:537–42. - PubMed
-
- Thom D. Variation in estimates of urinary incontinence prevalence in the community: effects of differences in definition, population characteristics, and study type. J Am Geriatr Soc. 1998;46:473–80. - PubMed
-
- Hampel C, Wienhold D, Benken N, Eggersmann C, Thuroff JW. Definition of overactive bladder and epidemiology of urinary incontinence. Urology. 1997;50(Suppl):4–14. - PubMed
-
- Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003;61:37–49. - PubMed
-
- Thom DH, Nygaard IE, Calhoun EA. Urologic Diseases in America Project: urinary incontinence in women — national trends in hospitalizations, office visits, treatment and economic impact. J Urol. 2005;173:1295–301. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U01 DK 58225/DK/NIDDK NIH HHS/United States
- U01 DK058234/DK/NIDDK NIH HHS/United States
- U01 DK58234/DK/NIDDK NIH HHS/United States
- U01 DK060393/DK/NIDDK NIH HHS/United States
- U01 DK60379/DK/NIDDK NIH HHS/United States
- U01 DK060380/DK/NIDDK NIH HHS/United States
- U01 DK060397/DK/NIDDK NIH HHS/United States
- U01 DK60380/DK/NIDDK NIH HHS/United States
- U01 DK60395/DK/NIDDK NIH HHS/United States
- U01 DK060401/DK/NIDDK NIH HHS/United States
- U01 DK060395/DK/NIDDK NIH HHS/United States
- U01 DK58229/DK/NIDDK NIH HHS/United States
- U01 DK60397/DK/NIDDK NIH HHS/United States
- U01 DK58231/DK/NIDDK NIH HHS/United States
- U01 DK60393/DK/NIDDK NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- U01 DK060379/DK/NIDDK NIH HHS/United States
- U01 DK60401/DK/NIDDK NIH HHS/United States
- U01 DK058229/DK/NIDDK NIH HHS/United States
- U01 DK58225/DK/NIDDK NIH HHS/United States
- U01 DK058225/DK/NIDDK NIH HHS/United States
- U01 DK058231/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous