

Treatment with apolipoprotein A-1 mimetic peptide reduces lupus-like manifestations in a murine lupus model of accelerated atherosclerosis
- PMID: 20482780
- PMCID: PMC2911877
- DOI: 10.1186/ar3020
Treatment with apolipoprotein A-1 mimetic peptide reduces lupus-like manifestations in a murine lupus model of accelerated atherosclerosis
Abstract
Introduction: The purpose of this study was to evaluate the effects of L-4F, an apolipoprotein A-1 mimetic peptide, alone or with pravastatin, in apoE-/-Fas-/-C57BL/6 mice that spontaneously develop immunoglobulin G (IgG) autoantibodies, glomerulonephritis, osteopenia, and atherosclerotic lesions on a normal chow diet.
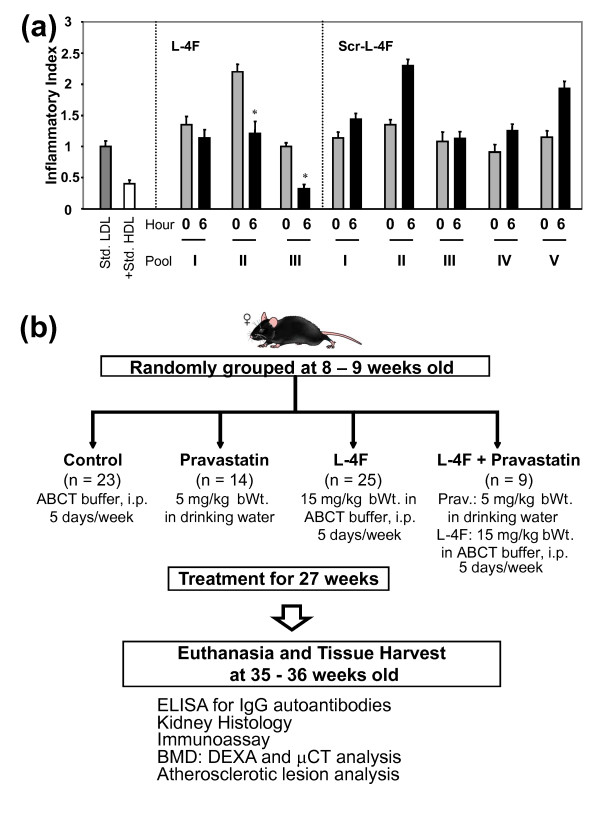
Methods: Female mice, starting at eight to nine weeks of age, were treated for 27 weeks with 1) pravastatin, 2) L-4F, 3) L-4F plus pravastatin, or 4) vehicle control, followed by disease phenotype assessment.
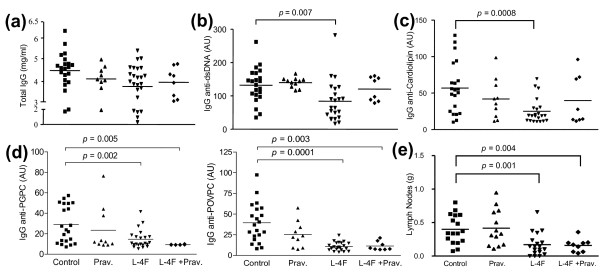
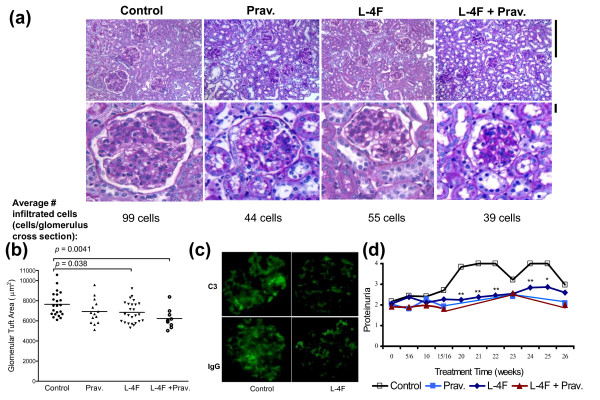
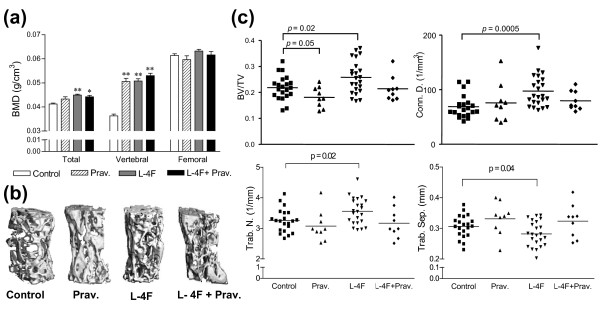
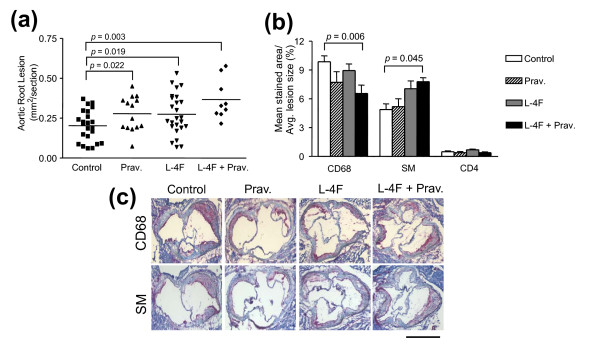
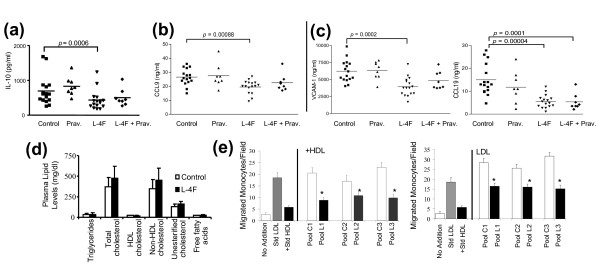
Results: In preliminary studies, dysfunctional, proinflammatory high-density lipoproteins (piHDL) were decreased six hours after a single L-4F, but not scrambled L-4F, injection in eight- to nine-week old mice. After 35 weeks, L-4F-treated mice, in the absence/presence of pravastatin, had significantly smaller lymph nodes and glomerular tufts (PL, LP<0.05), lower serum levels of IgG antibodies to double stranded DNA (dsDNA) (PL<0.05) and oxidized phospholipids (oxPLs) (PL, LP<0.005), and elevated total and vertebral bone mineral density (PL, LP<0.01) compared to vehicle controls. Although all treatment groups presented larger aortic root lesions compared to vehicle controls, enlarged atheromas in combination treatment mice had significantly less infiltrated CD68+ macrophages (PLP<0.01), significantly increased mean alpha-actin stained area (PLP<0.05), and significantly lower levels of circulating markers for atherosclerosis progression, CCL19 (PL, LP<0.0005) and VCAM-1 (PL<0.0002).
Conclusions: L-4F treatment, alone or with pravastatin, significantly reduced IgG anti-dsDNA and IgG anti-oxPLs, proteinuria, glomerulonephritis, and osteopenia in a murine lupus model of accelerated atherosclerosis. Despite enlarged aortic lesions, increased smooth muscle content, decreased macrophage infiltration, and decreased pro-atherogenic chemokines in L-4F plus pravastatin treated mice suggest protective mechanisms not only on lupus-like disease, but also on potential plaque remodeling in a murine model of systemic lupus erythematosus (SLE) and accelerated atherosclerosis.
Figures
Comment in
-
Sizing up stability: combination therapy with Apo-AI peptide mimetics and statins in systemic lupus erythematosus-mediated atherosclerosis.Arthritis Res Ther. 2010;12(5):139. doi: 10.1186/ar3115. Epub 2010 Sep 15. Arthritis Res Ther. 2010. PMID: 20854650 Free PMC article.
References
-
- Esdaile JM, Abrahamowicz M, Grodzicky T, Li Y, Panaritis C, du Berger R, Côte R, Grover SA, Fortin PR, Clarke AE, Senécal JL. Traditional Framingham risk factors fail to fully account for accelerated atherosclerosis in systemic lupus erythematosus. Arthritis and Rheumatism. 2001;44:2331–2337. doi: 10.1002/1529-0131(200110)44:10<2331::AID-ART395>3.0.CO;2-I. - DOI - PubMed
-
- Manzi S, Meilahn EN, Rairie JE, Conte CG, Medsger TA Jr, Jansen-McWilliams L, D'Agostino RB, Kuller LH. Age-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: comparison with the Framingham Study. Am J Epidemiol. 1997;145:408–415. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
