

Aldosterone-producing adenoma and other surgically correctable forms of primary aldosteronism
- PMID: 20482833
- PMCID: PMC2889888
- DOI: 10.1186/1750-1172-5-9
Aldosterone-producing adenoma and other surgically correctable forms of primary aldosteronism
Abstract
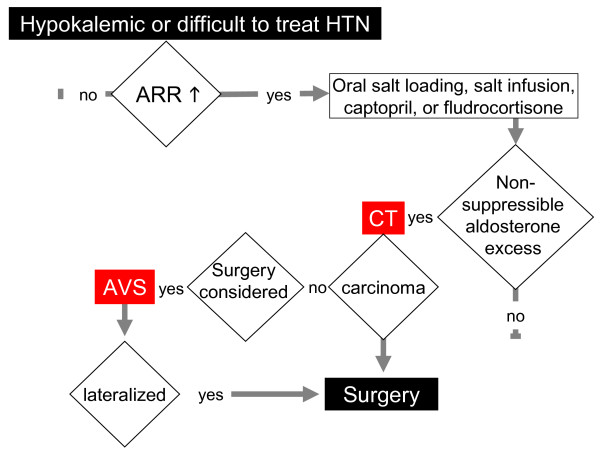
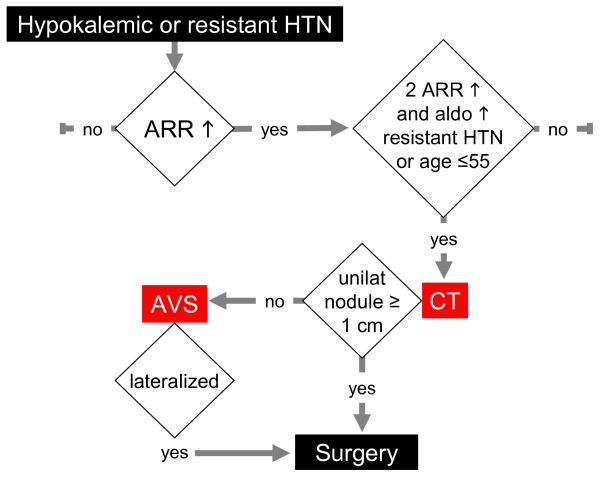
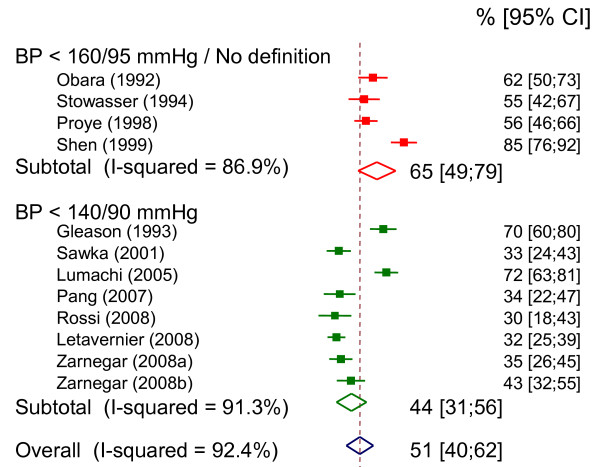
Surgically correctable forms of primary aldosteronism are characterized by unilateral aldosterone hypersecretion and renin suppression, associated with varying degrees of hypertension and hypokalemia. Unilateral aldosterone hypersecretion is caused by an aldosterone-producing adenoma (also known as Conn's adenoma and aldosteronoma), primary unilateral adrenal hyperplasia and rare cases of aldosterone-producing adrenocortical carcinoma. In these forms, unilateral adrenalectomy can cure aldosterone excess and hypokalemia, but not necessarily hypertension. The prevalence of primary aldosteronism in the general population is not known. Its prevalence in referred hypertensive populations is estimated to be between 6 and 13%, of which 1.5 to 5% have an aldosterone-producing adenoma or primary unilateral adrenal hyperplasia. Taking into account referral biases, the prevalence of surgically correctable primary aldosteronism is probably less than 1.5% in the hypertensive population and less than 0.3% in the general adult population. Surgically correctable primary aldosteronism is sought in patients with hypokalemic, severe or resistant forms of hypertension. Recent recommendations suggest screening for primary aldosteronism using the aldosterone to renin ratio. Patients with a raised ratio then undergo confirmatory suppression tests. The differential diagnosis of hypokalemic hypertension with low renin includes mineralocorticoid excess, with the mineralocorticoid being cortisol or 11-deoxycorticosterone, apparent mineralocorticoid excess, pseudo-hypermineralocorticoidism in Liddle syndrome or exposure to glycyrrhizic acid. Once the diagnosis is confirmed, adrenal computed tomography is performed for all patients. If surgery is considered, taking into consideration the clinical context and the desire of the patient, adrenal vein sampling is performed to detect whether or not aldosterone hypersecretion is unilateral. Laparoscopic surgery for unilateral aldosterone hypersecretion is associated with a morbidity of about 8%, with most complications being minor. It generally results in the normalization of aldosterone secretion and kalemia, and in a large decrease in blood pressure, but normotension without treatment is only achieved in half of all cases. Normotension following adrenalectomy is more frequent in young patients with recent hypertension than in patients with long-standing hypertension or a family history of hypertension.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
