

Race/ethnicity and potential suicide misclassification: window on a minority suicide paradox?
- PMID: 20482844
- PMCID: PMC2891687
- DOI: 10.1186/1471-244X-10-35
Race/ethnicity and potential suicide misclassification: window on a minority suicide paradox?
Abstract
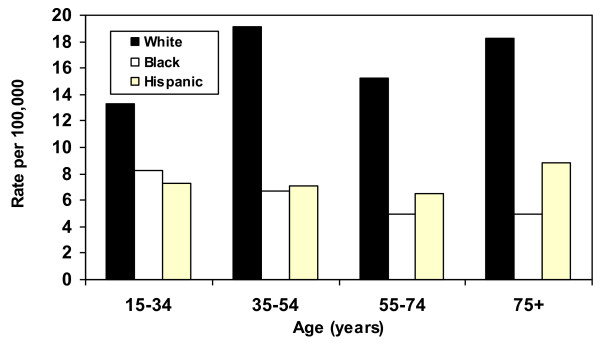
Background: Suicide officially kills approximately 30,000 annually in the United States. Analysis of this leading public health problem is complicated by undercounting. Despite persisting socioeconomic and health disparities, non-Hispanic Blacks and Hispanics register suicide rates less than half that of non-Hispanic Whites.
Methods: This cross-sectional study uses multiple cause-of-death data from the US National Center for Health Statistics to assess whether race/ethnicity, psychiatric comorbidity documentation, and other decedent characteristics were associated with differential potential for suicide misclassification. Subjects were 105,946 White, Black, and Hispanic residents aged 15 years and older, dying in the US between 2003 and 2005, whose manner of death was recorded as suicide or injury of undetermined intent. The main outcome measure was the relative odds of potential suicide misclassification, a binary measure of manner of death: injury of undetermined intent (includes misclassified suicides) versus suicide.
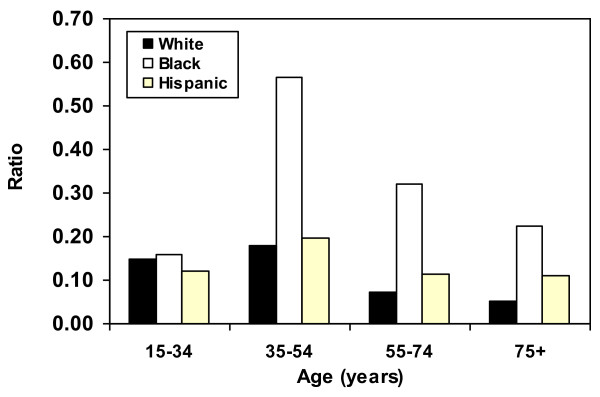
Results: Blacks (adjusted odds ratio [AOR], 2.38; 95% confidence interval [CI], 2.22-2.57) and Hispanics (1.17, 1.07-1.28) manifested excess potential suicide misclassification relative to Whites. Decedents aged 35-54 (AOR, 0.88; 95% CI, 0.84-0.93), 55-74 (0.52, 0.49-0.57), and 75+ years (0.51, 0.46-0.57) showed diminished misclassification potential relative to decedents aged 15-34, while decedents with 0-8 years (1.82, 1.75-1.90) and 9-12 years of education (1.43, 1.40-1.46) showed excess potential relative to the most educated (13+ years). Excess potential suicide misclassification was also apparent for decedents without (AOR, 3.12; 95% CI, 2.78-3.51) versus those with psychiatric comorbidity documented on their death certificates, and for decedents whose mode of injury was "less active" (46.33; 43.32-49.55) versus "more active."
Conclusions: Data disparities might explain much of the Black-White suicide rate gap, if not the Hispanic-White gap. Ameliorative action would extend from training in death certification to routine use of psychological autopsies in equivocal-manner-of-death cases.
Figures
References
-
- World Health Organization. Suicide Prevention (Supre) http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/ Accessed December 3, 2009.
-
- US Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System. http://www.cdc.gov/injury/wisqars/index.html Accessed December 3, 2009.
-
- Phillips DP, Ruth TE. Adequacy of official suicide statistics for scientific research and public policy. Suicide Life Threat Behav. 1993;23:307–319. - PubMed
-
- US Public Health Service. National Strategy for Suicide Prevention: Goals and Objectives for Action. Washington, DC: Department of Health and Human Services; 2001. p. 120. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
