

Unilateral cross bite treated by corticotomy-assisted expansion: two case reports
- PMID: 20482859
- PMCID: PMC2893126
- DOI: 10.1186/1746-160X-6-6
Unilateral cross bite treated by corticotomy-assisted expansion: two case reports
Abstract
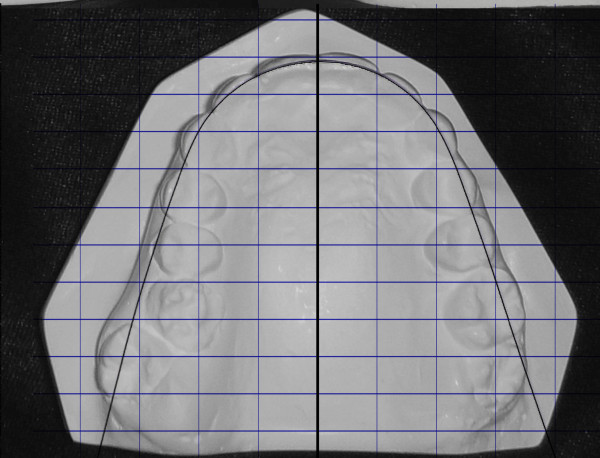
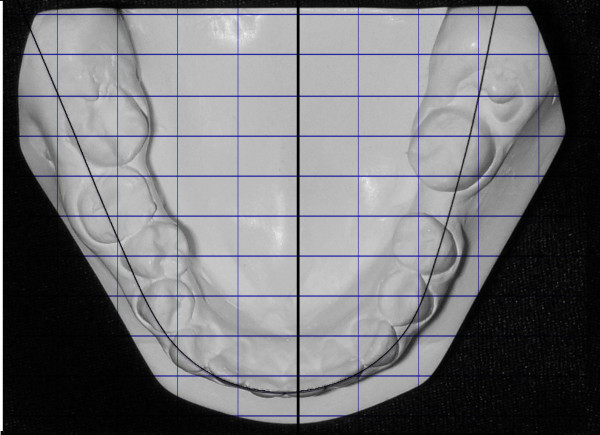
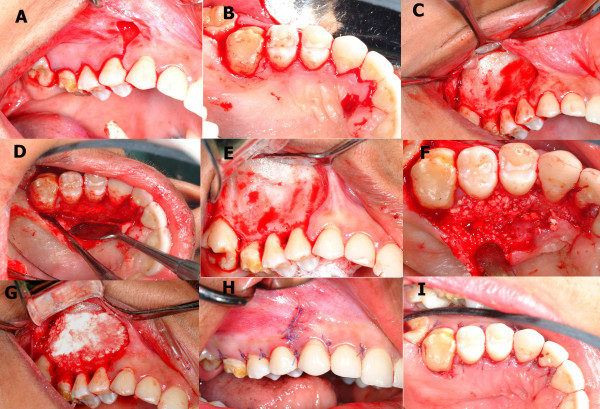
Background: True unilateral posterior crossbite in adults is a challenging malocclusion to treat. Conventional expansion methods are expected to have some shortcomings. The aim of this paper is to introduce a new technique for treating unilateral posterior crossbite in adults, namely, corticotomy-assisted expansion (CAE) applied on two adult patients: one with a true unilateral crossbite and the other with an asymmetrical bilateral crossbite, both treated via modified corticotomy techniques and fixed orthodontic appliances.
Methods: Two cases with asymmetric maxillary constriction were treated using CAE.
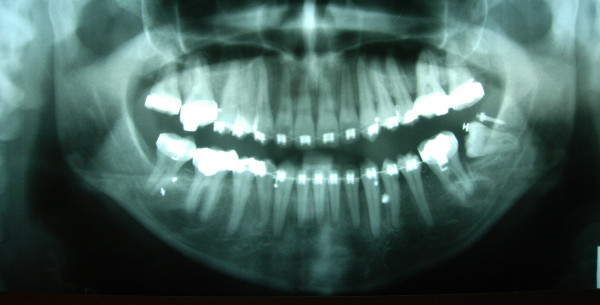
Results: In both cases, effective asymmetrical expansion was achieved using CAE, and functional occlusion was established as well.
Conclusions: Unilateral CAE presents an effective and reliable technique to treat true unilateral crossbite.
Figures

















Similar articles
-
Maxillary Orthodontic Expansion Assisted by Unilateral Alveolar Corticotomy and Low-Level Laser Therapy: A Novel Approach for Correction of a Posterior Unilateral Cross-Bite in Adults.J Lasers Med Sci. 2019 Summer;10(3):225-229. doi: 10.15171/jlms.2019.36. Epub 2019 Jul 6. J Lasers Med Sci. 2019. PMID: 31749950 Free PMC article.
-
Asymmetric maxillary expansion (AMEX) appliance for treatment of true unilateral posterior crossbite.Am J Orthod Dentofacial Orthop. 2002 Aug;122(2):164-73. doi: 10.1067/mod.2002.125563. Am J Orthod Dentofacial Orthop. 2002. PMID: 12165770 Clinical Trial.
-
Evaluation and comparison of stresses and displacements generated by four different types of asymmetric maxillary expansion appliances in true unilateral crossbite using finite element method.Int Orthod. 2022 Sep;20(3):100668. doi: 10.1016/j.ortho.2022.100668. Epub 2022 Jul 22. Int Orthod. 2022. PMID: 35879207
-
Comparison of effectiveness of quad helix appliance with other slow maxillary expanders in children with posterior crossbite: A systematic review.J Indian Soc Pedod Prev Dent. 2018 Jul-Sep;36(3):225-233. doi: 10.4103/JISPPD.JISPPD_85_17. J Indian Soc Pedod Prev Dent. 2018. PMID: 30246741
-
[Interceptive treatments (ages 6-10) of transverse deformities: posterior crossbite].Orthod Fr. 2006 Jun;77(2):249-52. doi: 10.1051/orthodfr/200677249. Orthod Fr. 2006. PMID: 16866123 Review. French.
Cited by
-
Alveolar bone changes after asymmetric rapid maxillary expansion.Angle Orthod. 2015 Sep;85(5):799-805. doi: 10.2319/090214.1. Epub 2014 Dec 5. Angle Orthod. 2015. PMID: 25478739 Free PMC article.
-
Maxillary Orthodontic Expansion Assisted by Unilateral Alveolar Corticotomy and Low-Level Laser Therapy: A Novel Approach for Correction of a Posterior Unilateral Cross-Bite in Adults.J Lasers Med Sci. 2019 Summer;10(3):225-229. doi: 10.15171/jlms.2019.36. Epub 2019 Jul 6. J Lasers Med Sci. 2019. PMID: 31749950 Free PMC article.
-
Three-Dimensional Prospective Evaluation of Piezocision-Assisted and Conventional Rapid Maxillary Expansion: A Controlled Clinical Trial.Open Access Maced J Med Sci. 2019 Jan 5;7(1):127-133. doi: 10.3889/oamjms.2019.021. eCollection 2019 Jan 15. Open Access Maced J Med Sci. 2019. PMID: 30740176 Free PMC article.
-
Effects of High Frequency Acceleration Device on Aligner Treatment-A Pilot Study.Dent J (Basel). 2018 Jul 12;6(3):32. doi: 10.3390/dj6030032. Dent J (Basel). 2018. PMID: 30002296 Free PMC article.
-
Periodontal Intervention in Speedy Orthodontics-A Case Report.J Clin Diagn Res. 2016 Jan;10(1):ZD15-6. doi: 10.7860/JCDR/2016/11425.7139. Epub 2016 Jan 1. J Clin Diagn Res. 2016. PMID: 26894189 Free PMC article.
References
-
- Thilander B, Myrberg N. The prevalence of malocclusion in Swedish schoolchildren. Scand J Dent Res. 1973;81:12–21. - PubMed
-
- Egermark-Eriksson I, Carlsson GE, Magnusson T, Thilander B. A longitudinal study on malocclusion in relation to signs and symptoms of cranio-mandibular disorders in children and adolescents. Eur J Orthod. 1990;12:399–407. - PubMed
-
- Heikenheimo KSK. Need for orthodontic intervention in five-year-old Finnish children. Proc Finn Dent Soc. 1987;83:165–169. - PubMed
-
- Proffit W. Contemporary orthodontics. 4. St Louis: C. V. Mosby; 2007.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
