

Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis
- PMID: 20483451
- PMCID: PMC3993088
- DOI: 10.1016/S0140-6736(10)60674-5
Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis
Abstract
Background: Substantial controversy surrounds the use of estimated glomerular filtration rate (eGFR) and albuminuria to define chronic kidney disease and assign its stages. We undertook a meta-analysis to assess the independent and combined associations of eGFR and albuminuria with mortality.
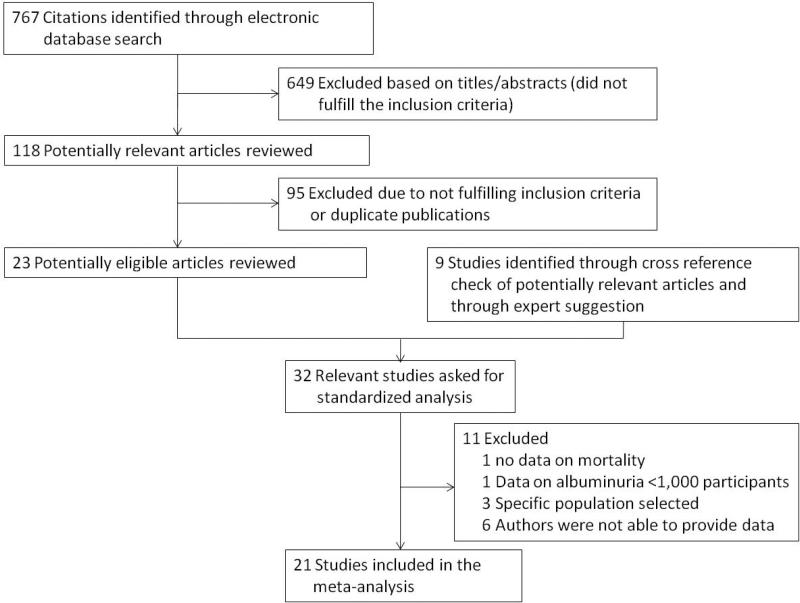
Methods: In this collaborative meta-analysis of general population cohorts, we pooled standardised data for all-cause and cardiovascular mortality from studies containing at least 1000 participants and baseline information about eGFR and urine albumin concentrations. Cox proportional hazards models were used to estimate hazard ratios (HRs) for all-cause and cardiovascular mortality associated with eGFR and albuminuria, adjusted for potential confounders.
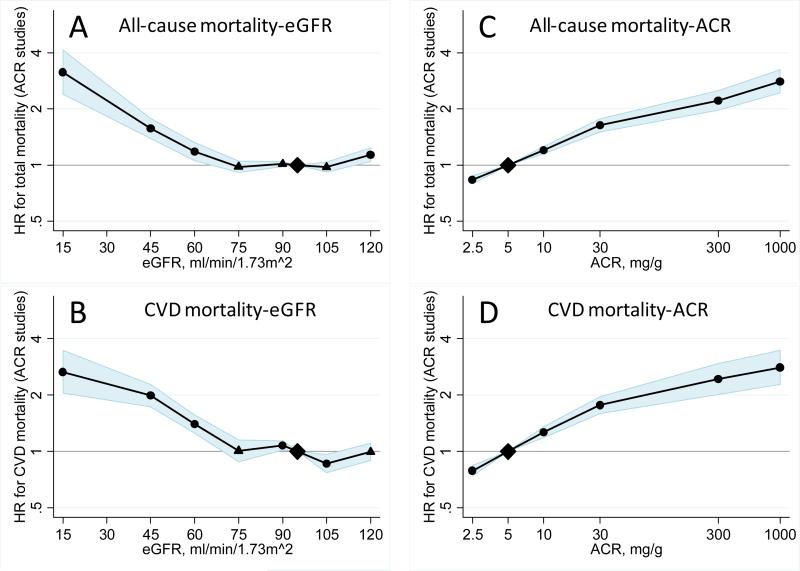
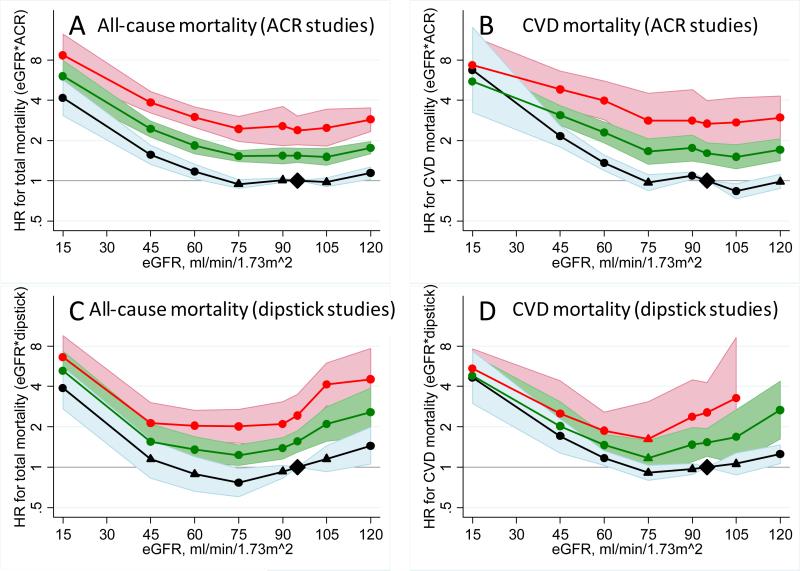
Findings: The analysis included 105,872 participants (730,577 person-years) from 14 studies with urine albumin-to-creatinine ratio (ACR) measurements and 1,128,310 participants (4,732,110 person-years) from seven studies with urine protein dipstick measurements. In studies with ACR measurements, risk of mortality was unrelated to eGFR between 75 mL/min/1.73 m(2) and 105 mL/min/1.73 m(2) and increased at lower eGFRs. Compared with eGFR 95 mL/min/1.73 m(2), adjusted HRs for all-cause mortality were 1.18 (95% CI 1.05-1.32) for eGFR 60 mL/min/1.73 m(2), 1.57 (1.39-1.78) for 45 mL/min/1.73 m(2), and 3.14 (2.39-4.13) for 15 mL/min/1.73 m(2). ACR was associated with risk of mortality linearly on the log-log scale without threshold effects. Compared with ACR 0.6 mg/mmol, adjusted HRs for all-cause mortality were 1.20 (1.15-1.26) for ACR 1.1 mg/mmol, 1.63 (1.50-1.77) for 3.4 mg/mmol, and 2.22 (1.97-2.51) for 33.9 mg/mmol. eGFR and ACR were multiplicatively associated with risk of mortality without evidence of interaction. Similar findings were recorded for cardiovascular mortality and in studies with dipstick measurements.
Interpretation: eGFR less than 60 mL/min/1.73 m(2) and ACR 1.1 mg/mmol (10 mg/g) or more are independent predictors of mortality risk in the general population. This study provides quantitative data for use of both kidney measures for risk assessment and definition and staging of chronic kidney disease.
Funding: Kidney Disease: Improving Global Outcomes (KDIGO), US National Kidney Foundation, and Dutch Kidney Foundation.
Copyright 2010 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Overall health assessment: a renal perspective.Lancet. 2010 Jun 12;375(9731):2053-4. doi: 10.1016/S0140-6736(10)60748-9. Epub 2010 May 17. Lancet. 2010. PMID: 20483450 No abstract available.
-
Meta-analysis confirms relationship between eGFR, albuminuria and risk of mortality.Nat Rev Nephrol. 2010 Sep;6(9):501. doi: 10.1038/nrneph.2010.105. Nat Rev Nephrol. 2010. PMID: 20815092 No abstract available.
References
-
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, et al. Chronic kidney disease as a global public health problem: approaches and initiatives - a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007;72:247–59. - PubMed
-
- National Kidney Foundation K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39:S1–266. - PubMed
-
- Wen CP, Cheng TY, Tsai MK, Chang YC, Chan HT, Tsai SP, et al. All-cause mortality attributable to chronic kidney disease: a prospective cohort study based on 462 293 adults in Taiwan. Lancet. 2008;371:2173–82. - PubMed
-
- Chadban SJ, Briganti EM, Kerr PG, Dunstan DW, Welborn TA, Zimmet PZ, et al. Prevalence of kidney damage in Australian adults: The AusDiab kidney study. J Am Soc Nephrol. 2003;14:S131–8. - PubMed
-
- Hallan SI, Coresh J, Astor BC, Asberg A, Powe NR, Romundstad S, et al. International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol. 2006;17:2275–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK035073/DK/NIDDK NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- N01 HC075150/HC/NHLBI NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- R01 AG007181/AG/NIA NIH HHS/United States
- R01 DK073217/DK/NIDDK NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- U01 NS041588/NS/NINDS NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- R01 AG020098/AG/NIA NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- K23 DK067303/DK/NIDDK NIH HHS/United States
- N01 HC085086/HC/NHLBI NIH HHS/United States
- R01 HL043232/HL/NHLBI NIH HHS/United States
- R01 AG015928/AG/NIA NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- K23 DK002904/DK/NIDDK NIH HHS/United States
- U10 EY006594/EY/NEI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- N01 HC015103/HC/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- R01 DK031801/DK/NIDDK NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- N01 HC085079/HC/NHLBI NIH HHS/United States
- R01 HL068140/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- R01 AG028507/AG/NIA NIH HHS/United States
- R01 AG027058/AG/NIA NIH HHS/United States
- N01 HC045133/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
