

Decreased cerebral cortical serotonin transporter binding in ecstasy users: a positron emission tomography/[(11)C]DASB and structural brain imaging study
- PMID: 20483717
- PMCID: PMC2912692
- DOI: 10.1093/brain/awq103
Decreased cerebral cortical serotonin transporter binding in ecstasy users: a positron emission tomography/[(11)C]DASB and structural brain imaging study
Abstract
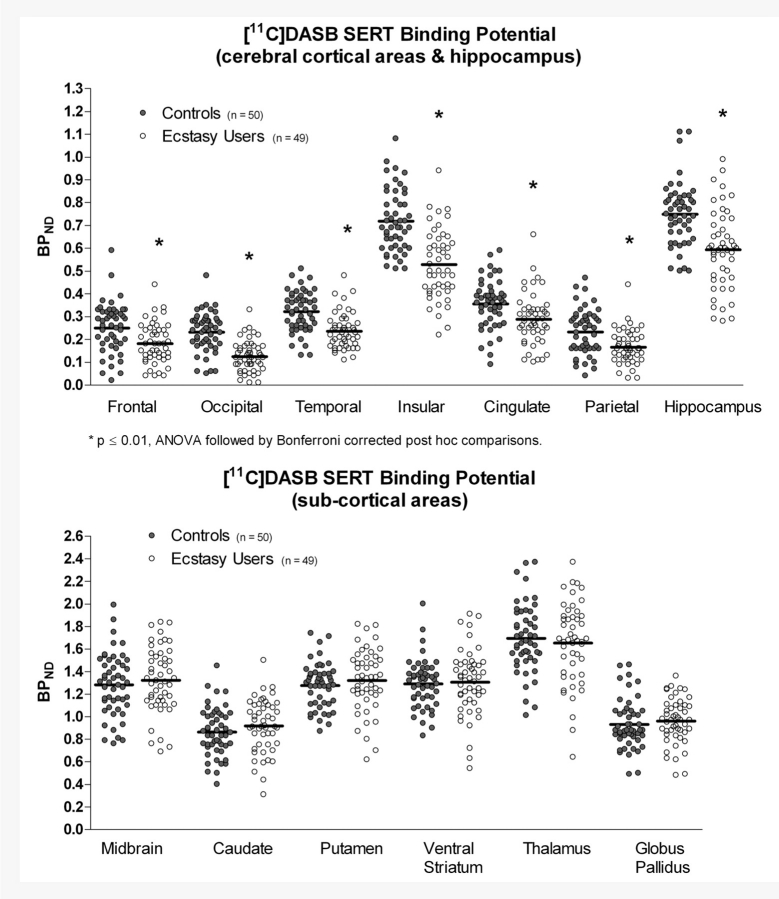
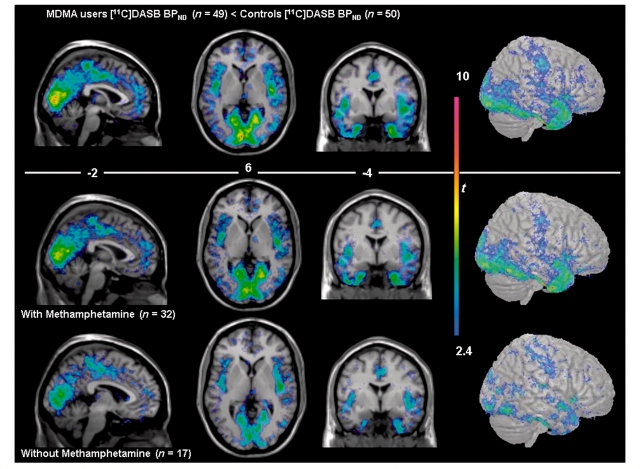
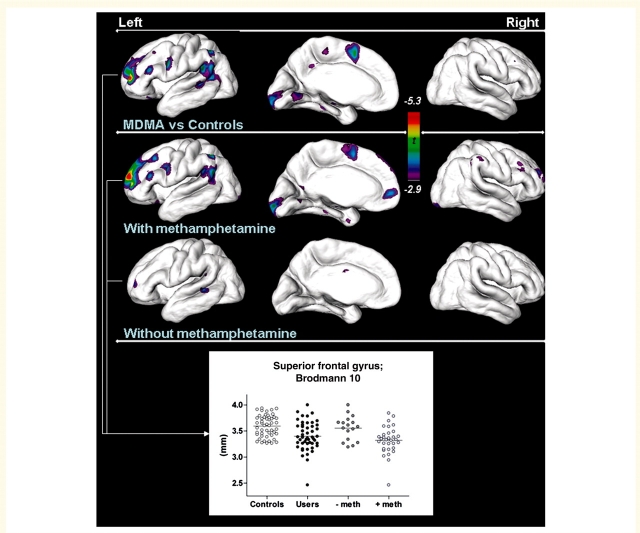
Animal data indicate that the recreational drug ecstasy (3,4-methylenedioxymethamphetamine) can damage brain serotonin neurons. However, human neuroimaging measurements of serotonin transporter binding, a serotonin neuron marker, remain contradictory, especially regarding brain areas affected; and the possibility that structural brain differences might account for serotonin transporter binding changes has not been explored. We measured brain serotonin transporter binding using [(11)C] N,N-dimethyl-2-(2-amino-4-cyanophenylthio) benzylamine in 50 control subjects and in 49 chronic (mean 4 years) ecstasy users (typically one to two tablets bi-monthly) withdrawn from the drug (mean 45 days). A magnetic resonance image for positron emission tomography image co-registration and structural analyses was acquired. Hair toxicology confirmed group allocation but also indicated use of other psychoactive drugs in most users. Serotonin transporter binding in ecstasy users was significantly decreased throughout all cerebral cortices (range -19 to -46%) and hippocampus (-21%) and related to the extent of drug use (years, maximum dose), but was normal in basal ganglia and midbrain. Substantial overlap was observed between control and user values except for insular cortex, in which 51% of ecstasy user values fell below the lower limit of the control range. Voxel-based analyses confirmed a caudorostral gradient of cortical serotonin transporter binding loss with occipital cortex most severely affected. Magnetic resonance image measurement revealed no overall regional volume differences between groups; however, a slight left-hemispheric biased cortical thinning was detected in methamphetamine-using ecstasy users. The serotonin transporter binding loss was not related to structural changes or partial volume effect, use of other stimulant drugs, blood testosterone or oestradiol levels, major serotonin transporter gene promoter polymorphisms, gender, psychiatric status, or self-reported hyperthermia or tolerance. The ecstasy group, although 'grossly behaviourally normal', reported subnormal mood and demonstrated generally modest deficits on some tests of attention, executive function and memory, with the latter associated with serotonin transporter decrease. Our findings suggest that the 'typical'/low dose (one to two tablets/session) chronic ecstasy-polydrug user might display a highly selective mild to marked loss of serotonin transporter in cerebral cortex/hippocampus in the range of that observed in Parkinson's disease, which is not gender-specific or completely accounted for by structural brain changes, recent use of other drugs (as assessed by hair analyses) or other potential confounds that we could address. The striking sparing of serotonin transporter-rich striatum (although possibly affected in 'heavier' users) suggests that serotonergic neurons innervating cerebral cortex are more susceptible, for unknown reasons, to ecstasy than those innervating subcortical regions and that behavioural problems in some ecstasy users during abstinence might be related to serotonin transporter changes limited to cortical regions.
Figures
References
-
- Ad-Dab'bagh Y, Einarson D, Lyttelton O, Muehlboeck JS, Mok K, Ivanov O, et al. The CIVET image-processing environment: a fully automated comprehensive pipeline for anatomical neuroimaging research. In: NeuroImage, editor. Organization for Human Brain Mapping. Italy: Florence; 2006.
-
- Ad-Dab'bagh Y, Singh V, Robbins S, Lerch J, Lyttelton O, Fombonne E, et al. Native space cortical thickness measurement and the absence of correlation to cerebral volume. In: Zilles K, editor. Organization for human brain mapping. Toronto, Canada: Neuroimage; 2005.
-
- Bailey DL, Young H, Bloomfield PM, Meikle SR, Glass D, Myers MJ, et al. ECAT ART—a continuously rotating PET camera: performance characteristics, initial clinical studies, and installation considerations in a nuclear medicine department. Eur J Nucl Med. 1997;24:6–15. - PubMed
-
- Boileau I, Guttman M, Rusjan P, Adams JR, Houle S, Tong J, et al. Decreased binding of the D3 dopamine receptor-preferring ligand [11C]-(+)-PHNO in drug-naive Parkinson's disease. Brain. 2009;132:1366–75. - PubMed
-
- Bouso JC, Doblin R, Farre M, Alcazar MA, Gomez-Jarabo G. MDMA-assisted psychotherapy using low doses in a small sample of women with chronic posttraumatic stress disorder. J Psychoactive Drugs. 2008;40:225–36. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
