

Timing of CD8+ T cell responses in relation to commencement of capillary leakage in children with dengue
- PMID: 20483770
- PMCID: PMC4340505
- DOI: 10.4049/jimmunol.0903262
Timing of CD8+ T cell responses in relation to commencement of capillary leakage in children with dengue
Abstract
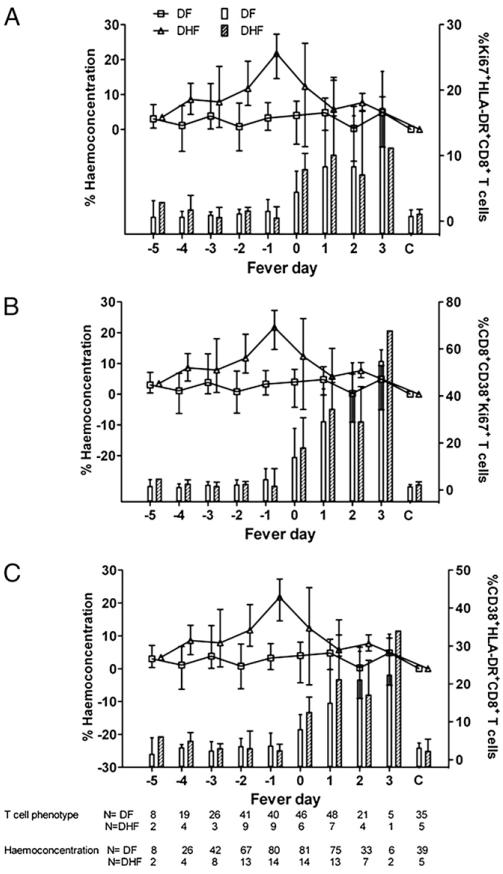
Immune activation is a feature of dengue hemorrhagic fever (DHF) and CD8+ T cell responses in particular have been suggested as having a role in the vasculopathy that characterizes this disease. By phenotyping CD8+ T cells (CD38+/HLA-DR+, CD38+/Ki-67+, or HLA-DR+/Ki-67+) in serial blood samples from children with dengue, we found no evidence of increased CD8+ T cell activation prior to the commencement of resolution of viremia or hemoconcentration. Investigations with MHC class I tetramers to detect NS3(133-142)-specific CD8+ T cells in two independent cohorts of children suggested the commencement of hemoconcentration and thrombocytopenia in DHF patients generally begins before the appearance of measurable frequencies of NS3(133-142)-specific CD8+ T cells. The temporal mismatch between the appearance of measurable surface activated or NS3(133-142)-specific CD8+ T cells suggests that these cells are sequestered at sites of infection, have phenotypes not detected by our approach, or that other mechanisms independent of CD8+ T cells are responsible for early triggering of capillary leakage in children with DHF.
Figures




References
-
- Srikiatkhachorn A, Krautrachue A, Ratanaprakarn W, Wongtapradit L, Nithipanya N, Kalayanarooj S, Nisalak A, Thomas SJ, Gibbons RV, Mammen MP, Jr., et al. Natural history of plasma leakage in dengue hemorrhagic fever: a serial ultrasonographic study. Pediatr. Infect. Dis. J. 2007;26:283–290. discussion 291-292. - PubMed
-
- Gamble J, Bethell D, Day NP, Loc PP, Phu NH, Gartside IB, Farrar JF, White NJ. Age-related changes in microvascular permeability: a significant factor in the susceptibility of children to shock? Clin. Sci. (Lond.) 2000;98:211–216. - PubMed
-
- Loke H, Bethell D, Phuong CX, Day N, White N, Farrar J, Hill A. Susceptibility to dengue hemorrhagic fever in Vietnam: evidence of an association with variation in the vitamin d receptor and Fc gamma receptor IIa genes. Am. J. Trop. Med. Hyg. 2002;67:102–106. - PubMed
-
- Loke H, Bethell DB, Phuong CX, Dung M, Schneider J, White NJ, Day NP, Farrar J, Hill AV. Strong HLA class I–restricted T cell responses in dengue hemorrhagic fever: a double-edged sword? J. Infect. Dis. 2001;184:1369–1373. - PubMed
-
- Graham RR, Juffrie M, Tan R, Hayes CG, Laksono I, Ma’roef C, Erlin, Sutary, Porter KR, Halstead SB. A prospective seroepidemiologic study on dengue in children four to nine years of age in Yogyakarta, Indonesia I. studies in 1995-1996. Am. J. Trop. Med. Hyg. 1999;61:412–419. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
