

Delivery of evidence-based treatment for multiple anxiety disorders in primary care: a randomized controlled trial
- PMID: 20483968
- PMCID: PMC2928714
- DOI: 10.1001/jama.2010.608
Delivery of evidence-based treatment for multiple anxiety disorders in primary care: a randomized controlled trial
Abstract
Context: Improving the quality of mental health care requires moving clinical interventions from controlled research settings into real-world practice settings. Although such advances have been made for depression, little work has been performed for anxiety disorders.
Objective: To determine whether a flexible treatment-delivery model for multiple primary care anxiety disorders (panic, generalized anxiety, social anxiety, and posttraumatic stress disorders) would be better than usual care (UC).
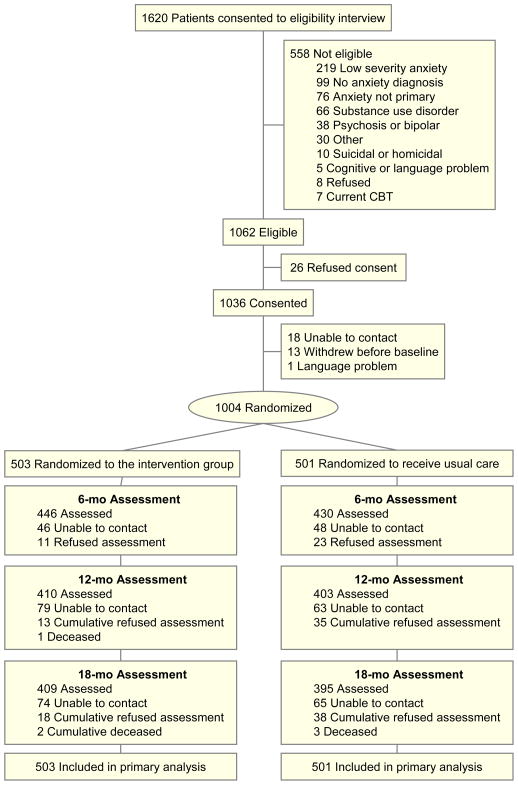
Design, setting, and patients: A randomized controlled effectiveness trial of Coordinated Anxiety Learning and Management (CALM) compared with UC in 17 primary care clinics in 4 US cities. Between June 2006 and April 2008, 1004 patients with anxiety disorders (with or without major depression), aged 18 to 75 years, English- or Spanish-speaking, were enrolled and subsequently received treatment for 3 to 12 months. Blinded follow-up assessments at 6, 12, and 18 months after baseline were completed in October 2009.
Intervention: CALM allowed choice of cognitive behavioral therapy (CBT), medication, or both; included real-time Web-based outcomes monitoring to optimize treatment decisions; and a computer-assisted program to optimize delivery of CBT by nonexpert care managers who also assisted primary care clinicians in promoting adherence and optimizing medications.
Main outcome measures: Twelve-item Brief Symptom Inventory (BSI-12) anxiety and somatic symptoms score. Secondary outcomes included proportion of responders (> or = 50% reduction from pretreatment BSI-12 score) and remitters (total BSI-12 score < 6).
Results: A significantly greater improvement for CALM vs UC in global anxiety symptoms was found (BSI-12 group mean differences of -2.49 [95% confidence interval {CI}, -3.59 to -1.40], -2.63 [95% CI, -3.73 to -1.54], and -1.63 [95% CI, -2.73 to -0.53] at 6, 12, and 18 months, respectively). At 12 months, response and remission rates (CALM vs UC) were 63.66% (95% CI, 58.95%-68.37%) vs 44.68% (95% CI, 39.76%-49.59%), and 51.49% (95% CI, 46.60%-56.38%) vs 33.28% (95% CI, 28.62%-37.93%), with a number needed to treat of 5.27 (95% CI, 4.18-7.13) for response and 5.50 (95% CI, 4.32-7.55) for remission.
Conclusion: For patients with anxiety disorders treated in primary care clinics, CALM compared with UC resulted in greater improvement in anxiety symptoms, depression symptoms, functional disability, and quality of care during 18 months of follow-up.
Trial registration: clinicaltrials.gov Identifier: NCT00347269.
Figures
Comment in
-
Coordinated multi-component treatment in primary care improves anxiety in adults with multiple anxiety disorders compared with usual care.Evid Based Ment Health. 2010 Nov;13(4):121. doi: 10.1136/ebmh.13.4.121. Evid Based Ment Health. 2010. PMID: 21036983 No abstract available.
References
-
- Westfall JM, Mold J, Fagnan L. Practice-based research--“Blue Highways” on the NIH roadmap. JAMA. 2007;297(4):403–406. - PubMed
-
- Unutzer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting. JAMA. 2002;288:2836–2845. - PubMed
-
- Wells KB, Sherbourne CD, Schoenbaum M, et al. Impact of disseminating quality improvement programs for depression in managed primary care: A randomized controlled trial. JAMA. 2000;283:212–220. - PubMed
-
- Katon W, Robinson P, Von Korff M, et al. A multifaceted intervention to improve treatment of depression in primary care. Arch Gen Psychiatry. 1996;53(10):924–932. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
