

Effect of adding a values clarification exercise to a decision aid on heart disease prevention: a randomized trial
- PMID: 20484089
- PMCID: PMC3996504
- DOI: 10.1177/0272989X10369008
Effect of adding a values clarification exercise to a decision aid on heart disease prevention: a randomized trial
Abstract
Background: Experts have called for the inclusion of values clarification (VC) exercises in decision aids (DAs) as a means of improving their effectiveness, but little research has examined the effects of such exercises.
Objective: To determine whether adding a VC exercise to a DA on heart disease prevention improves decision-making outcomes.
Design: Randomized trial.
Setting: UNC Decision Support Laboratory.
Patients: Adults ages 40 to 80 with no history of cardiovascular disease.
Intervention: A Web-based heart disease prevention DA with or without a VC exercise.
Measurements: Pre- and postintervention decisional conflict and intent to reduce coronary heart disease (CHD) risk and postintervention self-efficacy and perceived values concordance.
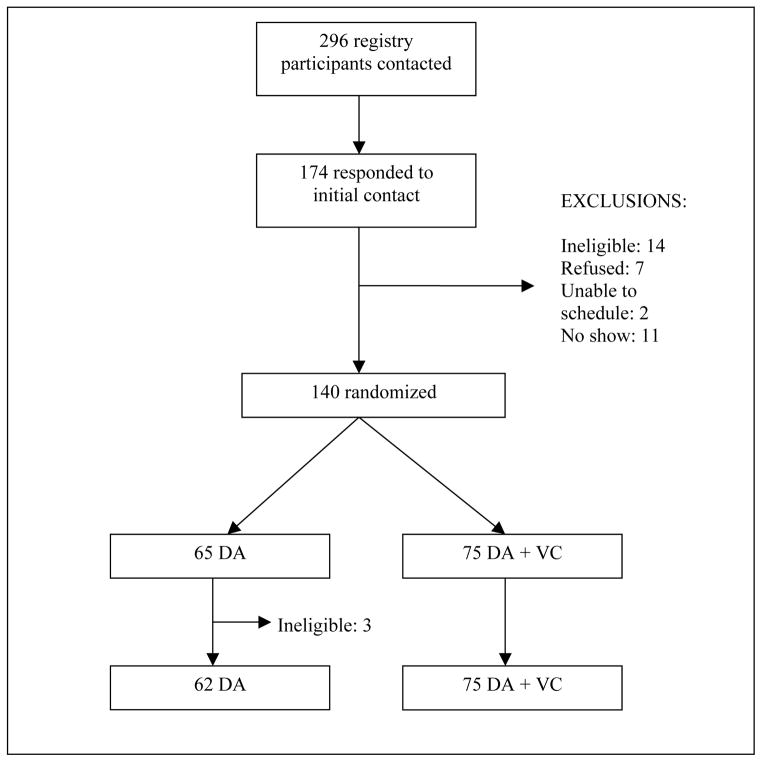
Results: The authors enrolled 137 participants (62 in DA; 75 in DA + VC with moderate decisional conflict (DA 2.4; DA + VC 2.5) and no baseline differences among groups. After the interventions, they found no clinically or statistically significant differences between groups in decisional conflict (DA 1.8; DA + VC 1.9; absolute difference VC-DA 0.1, 95% confidence interval [CI]: -0.1 to 0.3), intent to reduce CHD risk (DA 98%; DA + VC 100%; absolute difference VC-DA: 2%, 95% CI: -0.02% to 5%), perceived values concordance (DA 95%; DA + VC 92%; absolute difference VC-DA -3%, 95% CI: -11% to +5%), or self-efficacy for risk reduction (DA 97%; DA + VC 92%; absolute difference VC-DA -5%, 95% CI: -13% to +3%). However, DA + VC tended to change some decisions about risk reduction strategies.
Limitations: Use of a hypothetical scenario; ceiling effects for some outcomes.
Conclusions: Adding a VC intervention to a DA did not further improve decision-making outcomes in a population of highly educated and motivated adults responding to scenario-based questions. Work is needed to determine the effects of VC on more diverse populations and more distal outcomes.
Figures




References
-
- Sheridan SL, Harris RP, Woolf SH. Shared decision making about screening and chemoprevention. a suggested approach from the U.S. Preventive Services Task Force. Am J Prev Med. 2004;26(1):56–66. - PubMed
-
- O’Connor AM, Stacey D, Entwistle V, Llewellyn-Thomas H, Rovner D, Holmes-Rovner M, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2003;(2):CD001431. - PubMed
-
- O’Connor AM, Bennett CL, Stacey D, Barry M, Col NF, Eden KB, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2009;(3):CD001431. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
