

Incidental pancreatic cysts: do we really know what we are watching?
- PMID: 20484954
- PMCID: PMC3214832
- DOI: 10.1159/000243733
Incidental pancreatic cysts: do we really know what we are watching?
Abstract
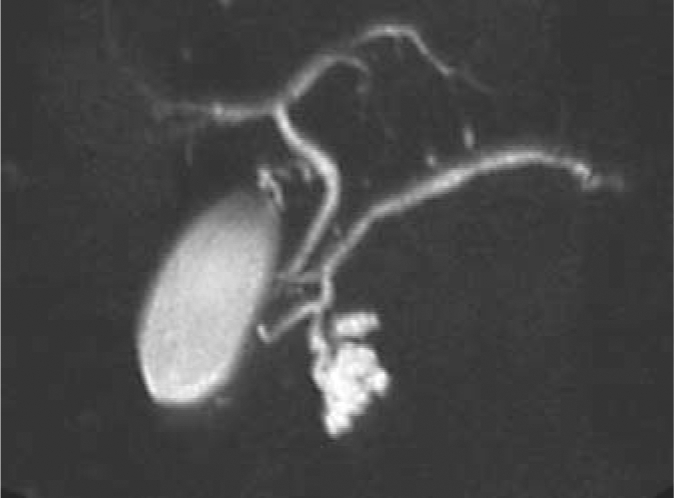
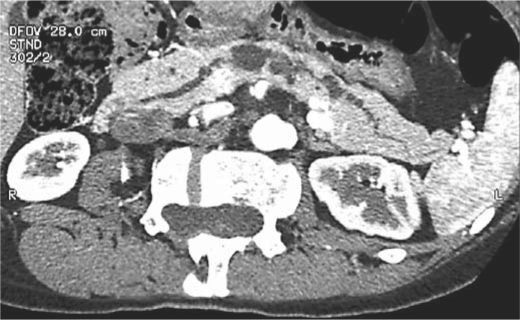
Background: Most cystic neoplasms of the pancreas (CNPs) are incidentally discovered. Their management continues to be debated and preoperative diagnosis is often inaccurate.
Methods: Retrospective review of 330 patients with incidentally discovered CNPs. Preoperative and final histological diagnoses were correlated.
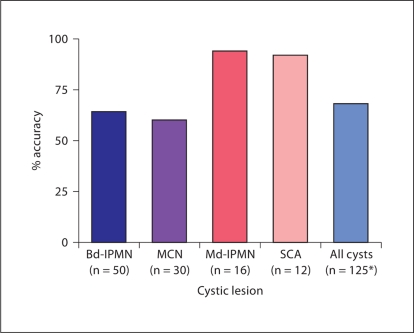
Results: 41% (136/330) of patients were operated on at diagnosis. 50 patients underwent resection for a presumed branch-duct (Bd) intraductal papillary mucinous neoplasm (IPMN), which was confirmed in only 64% (32/50); of the remaining patients, 20% had main-duct involvement. Mucinous cystic neoplasm was the preoperative diagnosis in 30/136 patients, histologic examination was confirmatory in only 60% (18/30). Most lesions presumed to be main-duct or combined IPMNs or serous cystadenomas were confirmed as such after resection (15/16 and 11/12, respectively). Multifocality was not only associated with Bd-IPMN, and 5% of all cysts were non-neoplastic. Overall, in only 68% of cases did the preoperative and histological diagnoses match.
Conclusions: In an experienced, high-volume center, preoperative diagnosis was incorrect in one-third of incidentally discovered CNPs who underwent resection. Of particular concern, 20% of presumed Bd-IPMN had a main-duct component. Conversely, 5% of resected cysts were not even neoplastic. Clearly, better diagnostic methods are needed to aid in formulating appropriate treatment strategies.
Copyright 2010 S. Karger AG, Basel.
Figures

Comment in
-
Management of pancreatic cystic neoplasms: decision-making with limited information.Pancreatology. 2010;10(2-3):142-3. doi: 10.1159/000276894. Epub 2010 May 12. Pancreatology. 2010. PMID: 20460945 No abstract available.
Similar articles
-
Evaluation of the guidelines for management of pancreatic branch-duct intraductal papillary mucinous neoplasm.Clin Gastroenterol Hepatol. 2008 Jul;6(7):815-9; quiz 719. doi: 10.1016/j.cgh.2008.04.005. Clin Gastroenterol Hepatol. 2008. PMID: 18602036
-
Pancreatic main-duct involvement in branch-duct IPMNs: an underestimated risk.Ann Surg. 2014 Nov;260(5):848-55; discussion 855-6. doi: 10.1097/SLA.0000000000000980. Ann Surg. 2014. PMID: 25379856
-
Long-term Risk of Pancreatic Malignancy in Patients With Branch Duct Intraductal Papillary Mucinous Neoplasm in a Referral Center.Gastroenterology. 2017 Nov;153(5):1284-1294.e1. doi: 10.1053/j.gastro.2017.07.019. Epub 2017 Jul 21. Gastroenterology. 2017. PMID: 28739282
-
[Intraductal papillary mucinous neoplasm of the pancreas (IPMN)--standards and new aspects].Zentralbl Chir. 2014 Jun;139(3):308-17. doi: 10.1055/s-0033-1350892. Epub 2013 Nov 15. Zentralbl Chir. 2014. PMID: 24241954 Review. German.
-
[Branch duct intraductal papillary mucinous neoplasm - contra resection].Chirurg. 2017 Nov;88(11):918-926. doi: 10.1007/s00104-017-0495-z. Chirurg. 2017. PMID: 28871376 Review. German.
Cited by
-
Pearls and pitfalls of imaging features of pancreatic cystic lesions: a case-based approach with imaging-pathologic correlation.Jpn J Radiol. 2021 Feb;39(2):118-142. doi: 10.1007/s11604-020-01032-1. Epub 2020 Aug 25. Jpn J Radiol. 2021. PMID: 32840742 Review.
-
Diagnostic accuracy of cyst fluid amphiregulin in pancreatic cysts.BMC Gastroenterol. 2012 Feb 14;12:15. doi: 10.1186/1471-230X-12-15. BMC Gastroenterol. 2012. PMID: 22333441 Free PMC article.
-
Not all mixed-type intraductal papillary mucinous neoplasms behave like main-duct lesions: implications of minimal involvement of the main pancreatic duct.Surgery. 2014 Sep;156(3):611-21. doi: 10.1016/j.surg.2014.04.023. Epub 2014 Jul 28. Surgery. 2014. PMID: 25081232 Free PMC article.
-
Endoscopic ultrasound-guided through-the-needle microforceps biopsy in the evaluation of pancreatic cystic lesions: a multicenter study.Endosc Int Open. 2018 Dec;6(12):E1423-E1430. doi: 10.1055/a-0770-2700. Epub 2018 Dec 5. Endosc Int Open. 2018. PMID: 30574535 Free PMC article.
-
Diagnostic Concordance and Preoperative Risk Factors for Malignancy in Pancreatic Mucinous Cystic Neoplasms.Gut Liver. 2022 Jul 15;16(4):637-644. doi: 10.5009/gnl210231. Epub 2021 Dec 21. Gut Liver. 2022. PMID: 34933278 Free PMC article.
References
-
- Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M, Yamaguchi K, Yamao K, Matsuno S. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6:17–32. - PubMed
-
- Das A, Wells CD, Nguyen CC. Incidental cystic neoplasms of pancreas: what is the optimal interval of imaging surveillance? Am J Gastroenterol. 2008;103:1657–1662. - PubMed
-
- Glantz SA. Primer of Biostatistics. ed 6. New York: McGraw-Hill Medical; 2005.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
