

Meta-analyses of the effect of symptoms of gastroesophageal reflux on the risk of Barrett's esophagus
- PMID: 20485283
- PMCID: PMC2916949
- DOI: 10.1038/ajg.2010.194
Meta-analyses of the effect of symptoms of gastroesophageal reflux on the risk of Barrett's esophagus
Abstract
Objectives: Esophageal adenocarcinoma (EAC) is a devastating disease that has risen in incidence over the past several decades. Barrett's esophagus (BE) is an associated premalignant lesion. Current preventative efforts rely on endoscopic screening of individuals with gastroesophageal reflux disease (GERD) symptoms and surveillance endoscopy for those with BE. However, some recent studies have found a high prevalence of BE in patients without GERD, and others have found little or no association with GERD. We hypothesized that studies of higher-quality design show weaker associations of GERD with BE, and that GERD is only weakly associated with short-segment Barrett's esophagus (SSBE).
Methods: We performed a systematic literature search in multiple online electronic databases regardless of language. Eligible studies required visualization of columnar mucosa and histological confirmation of intestinal metaplasia, and GERD symptoms ascertained by questionnaire or interview. The highest-quality sampling design was defined a priori by both cases and controls identified among unselected research volunteers ("research design") rather than by patients selected for endoscopy for clinical indications ("clinical design"), which introduces selection and ascertainment bias. A priori, heterogeneity was defined by Cochrane's Q P<0.20 and the inconsistency index (I(2); 25% low, 50% moderate, and 75% high). Heterogeneity of results can reflect significant differences in study design or effect modification by strata of outcomes.
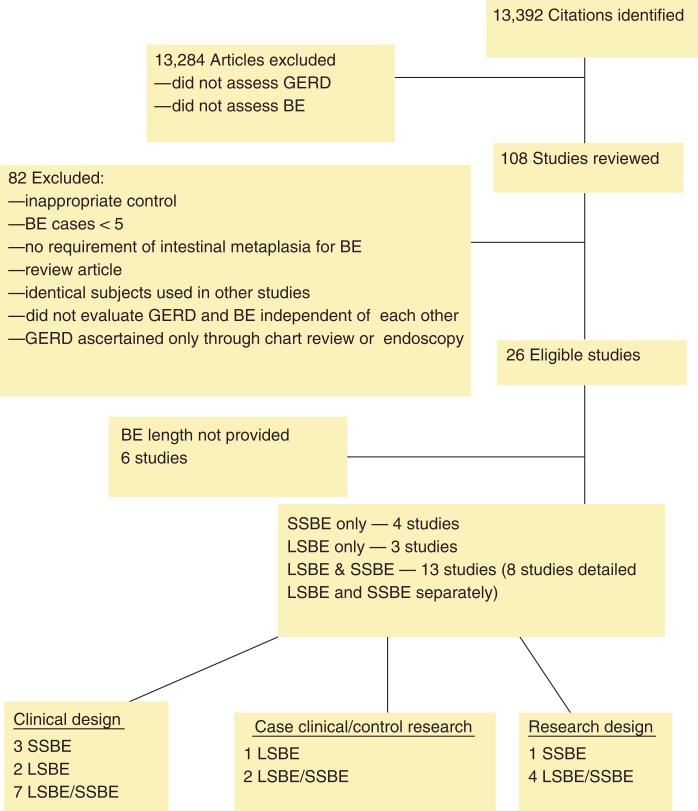
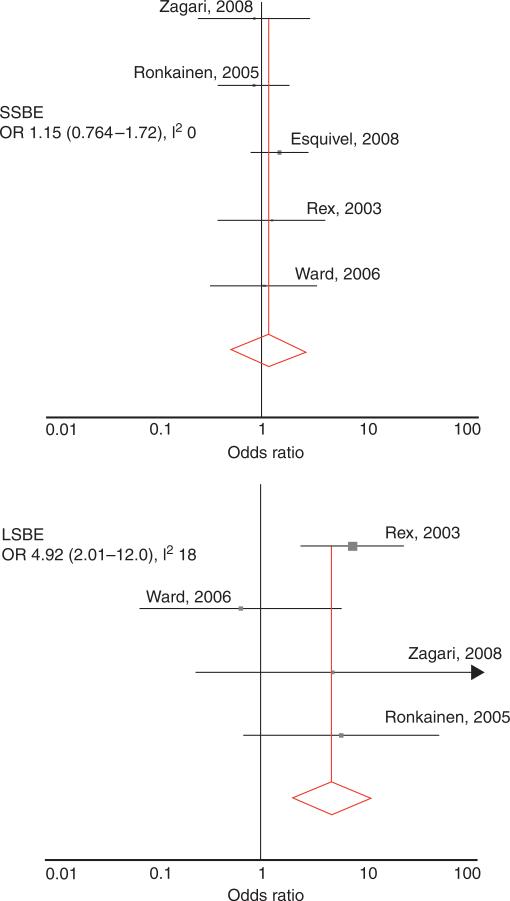
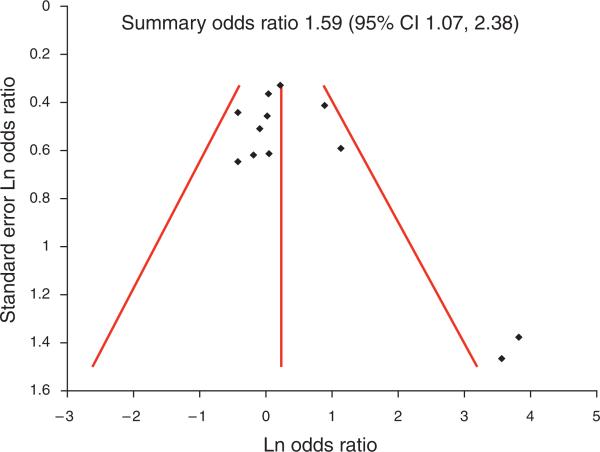
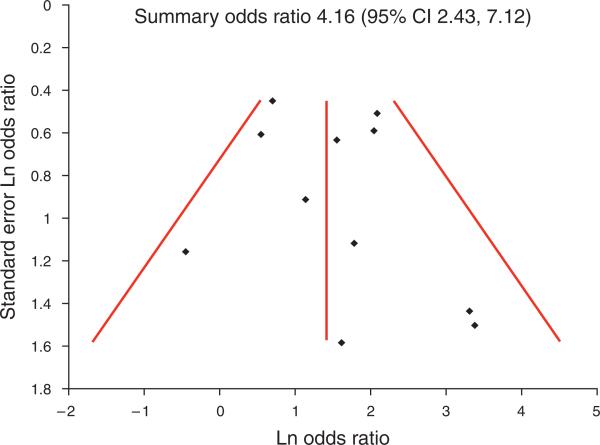
Results: Systematic review identified 13,392 citations. Evaluation identified 108 potentially relevant journal articles, of which 26 met eligibility. Of these, 14 studies identified cases of BE and controls based on clinical indication ("clinical design"), and 6 used the "research design." The remaining six studies identified cases of BE from patients undergoing endoscopy for clinical indication and controls among patients without known BE ("cases clinical/controls research"). The summary odds ratio (OR) for the association of GERD with BE from all studies was 2.90 (95% confidence interval (CI), 1.86-4.54), but the results were very heterogeneous (P=0.0001; I(2)=89%). When stratified by BE length and sampling design, the studies with clinical design showed substantial, but heterogeneous, associations with SSBE (OR, 2.38; 95% CI, 1.21-4.70; P=0.02; I(2)=62%), and stronger and homogeneous association with long-segment BE (LSBE; fixed effects OR, 2.96; 95% CI, 1.69-5.19; P=0.25; I(2)=25%). In the research study design, stratifying by length of BE resolved the heterogeneity and showed a strong association between GERD and LSBE (fixed effects OR, 4.92; 95% CI, 2.01-12.0; P=0.30; I(2)=19%) and no association with SSBE (fixed effects OR, 1.15; 95% CI, 0.763-1.73; P=0.84; I(2)=0%). Funnel plots showed potential evidence for bias against dissemination of small negative studies.
Conclusions: In the highest-quality studies, GERD symptoms are not associated with SSBE, but increased the odds of LSBE by fivefold. GERD symptoms can serve as a reliable predictor of LSBE, but not SSBE. If SSBE is considered worthy of identification, then current screening practices do not select patients at risk for endoscopy, and alternative methods of selection for screening need to be developed.
Figures
References
-
- Bytzer P, Christensen PB, Damkier P, et al. Adenocarcinoma of the esophagus and Barrett's esophagus: a population-based study. Am J Gastroenterol. 1999;94:86. - PubMed
-
- Pohl H, Welch HG. The role of over diagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97:142–6. - PubMed
-
- Lagergren J. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999;340:825. - PubMed
-
- Chak A, Faulx A, Eng C, et al. Gastroesophageal reflux symptoms in patients with adenocarcinoma of the esophagus or cardia. Cancer. 2006;107:2160. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
