

Giant hyperplasia of the caudate lobe in a patient with liver cirrhosis: case report and literature review
- PMID: 20485648
- PMCID: PMC2871638
- DOI: 10.5009/gnl.2008.2.3.205
Giant hyperplasia of the caudate lobe in a patient with liver cirrhosis: case report and literature review
Abstract
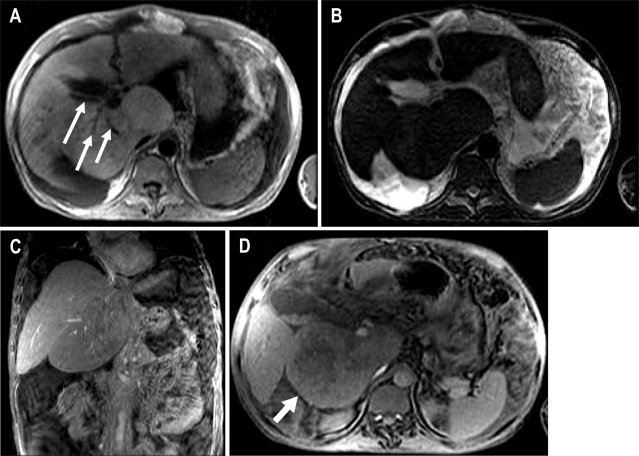
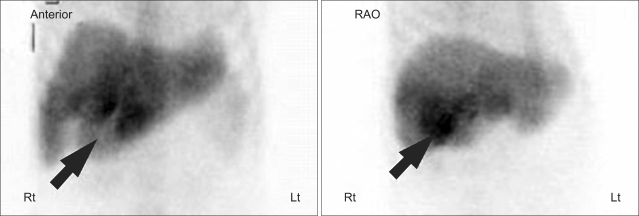
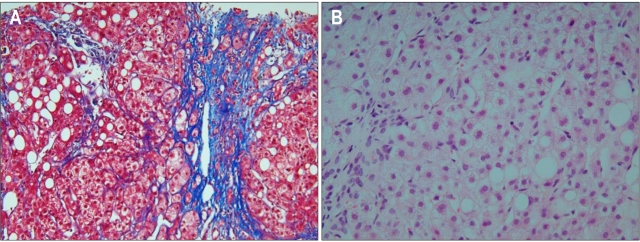
The caudate lobe often exhibits enlargement and nodularity in cases of cirrhosis, which makes differentiation of hepatocellular carcinoma from other mass-like lesions of the caudate lobe difficult in cirrhotic patients. A 12x6 cm mass-like enlargement of the caudate lobe was incidentally found by computed tomography in a 38-year-old man suffering from alcoholic liver cirrhosis. Magnetic resonance imaging, liver colloidal scan, and sonoguided liver biopsy were used for the differential diagnosis. A literature review revealed two case reports, all of which (like ours) presented with an enlarged caudate lobe supplied with blood via a branch of the portal vein. Therefore, in cases of giant hyperplasia of the caudate lobe, confirmation of the caudate lobe blood supply and the enhancement pattern might be important for the differentiation.
Keywords: Caudate lobe; Cirrhosis; Giant hyperplasia.
Figures
Similar articles
-
Giant hyperplasia of the caudate lobe of the cirrhotic liver: correlation with an anomaly of the caudate portal branch.Abdom Imaging. 1999 Mar-Apr;24(2):153-6. doi: 10.1007/s002619900465. Abdom Imaging. 1999. PMID: 10024401
-
Pseudotumorous enlargement of the paracaval portion of the caudate lobe: a report of two cases with CT and MR appearance.Abdom Imaging. 1997 Jul-Aug;22(4):398-400. doi: 10.1007/s002619900219. Abdom Imaging. 1997. PMID: 9157859
-
Pseudotumorous hyperplasia of the caudate lobe in the non-cirrhotic liver: MR and CT arterial portography appearance.Hepatogastroenterology. 2000 Jul-Aug;47(34):909-11. Hepatogastroenterology. 2000. PMID: 11020845
-
Human liver caudate lobe and liver segment.Anat Sci Int. 2002 Dec;77(4):211-24. doi: 10.1046/j.0022-7722.2002.00033.x. Anat Sci Int. 2002. PMID: 12557417 Review.
-
Selective Chemoembolization of Caudate Lobe Hepatocellular Carcinoma: Anatomy and Procedural Techniques.Radiographics. 2019 Jan-Feb;39(1):289-302. doi: 10.1148/rg.2019180110. Radiographics. 2019. PMID: 30620696 Review.
Cited by
-
Does providing routine liver volume assessment add value when performing CT surveillance in cirrhotic patients?Abdom Radiol (NY). 2019 Oct;44(10):3263-3272. doi: 10.1007/s00261-019-02145-6. Abdom Radiol (NY). 2019. PMID: 31359098 Free PMC article.
References
-
- Torres WE, Whitmire LF, Gedgaudas-McClees K, Bernardino ME. Computed tomography of hepatic morphologic changes in cirrhosis of the liver. J Comput Assist Tomogr. 1986;10:47–50. - PubMed
-
- Kerlin P, Davis GL, McGill DB, Weiland LH, Adson MA, Sheedy PF., 2nd Hepatic adenoma and focal nodular hyperplasia: clinical, pathologic, and radiologic features. Gastroenterology. 1983;84:994–1002. - PubMed
-
- Mathieu D, Vasile N, Menu Y, Van Beers B, Lorphelin JM, Pringot J. Budd-Chiari syndrome: dynamic CT. Radiology. 1987;165:409–413. - PubMed
-
- Vogelzang RL, Anschuetz SL, Gore RM. Budd-Chiari syndrome: CT observations. Radiology. 1987;163:329–333. - PubMed
-
- Awaya H, Mitchell DG, Kamishima T, Holland G, Ito K, Matsumoto T. Cirrhosis: modified caudate-right lobe ratio. Radiology. 2002;224:769–774. - PubMed
LinkOut - more resources
Full Text Sources
