

Patient retention and adherence to antiretrovirals in a large antiretroviral therapy program in Nigeria: a longitudinal analysis for risk factors
- PMID: 20485670
- PMCID: PMC2868044
- DOI: 10.1371/journal.pone.0010584
Patient retention and adherence to antiretrovirals in a large antiretroviral therapy program in Nigeria: a longitudinal analysis for risk factors
Abstract
Background: Substantial resources and patient commitment are required to successfully scale-up antiretroviral therapy (ART) and provide appropriate HIV management in resource-limited settings. We used pharmacy refill records to evaluate risk factors for loss to follow-up (LTFU) and non-adherence to ART in a large treatment cohort in Nigeria.
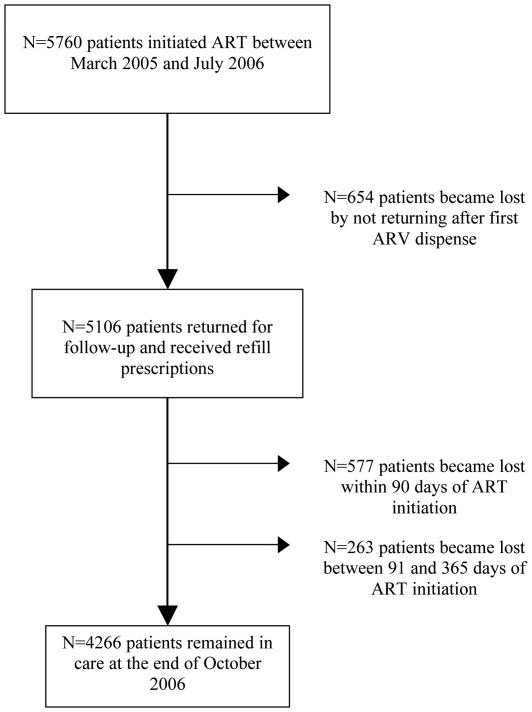
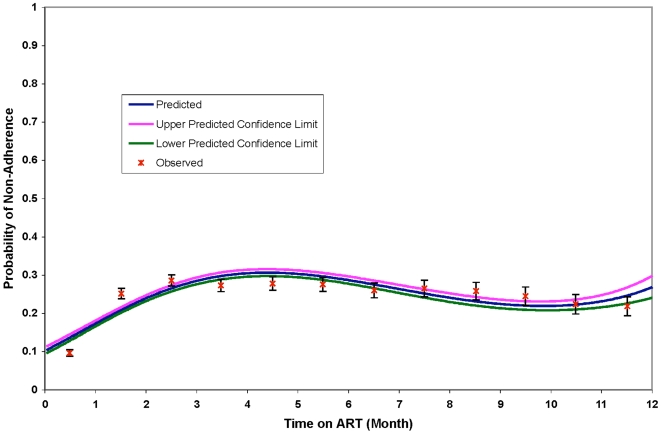
Methods and findings: We reviewed clinic records of adult patients initiating ART between March 2005 and July 2006 at five health facilities. Patients were classified as LTFU if they did not return >60 days from their expected visit. Pharmacy refill rates were calculated and used to assess non-adherence. We identified risk factors associated with LTFU and non-adherence using Cox and Generalized Estimating Equation (GEE) regressions, respectively. Of 5,760 patients initiating ART, 26% were LTFU. Female gender (p < 0.001), post-secondary education (p = 0.03), and initiating treatment with zidovudine-containing (p = 0.004) or tenofovir-containing (p = 0.05) regimens were associated with decreased risk of LTFU, while patients with only primary education (p = 0.02) and those with baseline CD4 counts (cell/ml(3)) >350 and <100 were at a higher risk of LTFU compared to patients with baseline CD4 counts of 100-200. The adjusted GEE analysis showed that patients aged <35 years (p = 0.005), who traveled for >2 hours to the clinic (p = 0.03), had total ART duration of >6 months (p<0.001), and CD4 counts >200 at ART initiation were at a higher risk of non-adherence. Patients who disclosed their HIV status to spouse/family (p = 0.01) and were treated with tenofovir-containing regimens (p < or = 0.001) were more likely to be adherent.
Conclusions: These findings formed the basis for implementing multiple pre-treatment visit preparation that promote disclosure and active community outreaching to support retention and adherence. Expansion of treatment access points of care to communities to diminish travel time may have a positive impact on adherence.
Conflict of interest statement
Figures
References
-
- UNAIDS. Geneva: UNAIDS/WHO; 2008. Epidemiologic Fact Sheet on HIV and AIDS - Nigeria - 2008 Update.
-
- Karcher H, Omondi A, Odera J, Kunz A, Harms G. Risk factors for treatment denial and loss to follow-up in an antiretroviral treatment cohort in Kenya. Trop Med Int Health. 2007;12:687–694. - PubMed
-
- Nacher M, El Guedj M, Vaz T, Nasser V, Randrianjohany A, et al. Risk factors for follow-up interruption of HIV patients in French Guiana. Am J Trop Med Hyg. 2006;74:915–917. - PubMed
-
- Krebs DW, Chi BH, Mulenga Y, Morris M, Cantrell RA, et al. Community-based follow-up for late patients enrolled in a district-wide programme for antiretroviral therapy in Lusaka, Zambia. AIDS Care. 2008;20:311–317. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
