

Phase I/II study of oncolytic herpes simplex virus NV1020 in patients with extensively pretreated refractory colorectal cancer metastatic to the liver
- PMID: 20486770
- PMCID: PMC3733135
- DOI: 10.1089/hum.2010.020
Phase I/II study of oncolytic herpes simplex virus NV1020 in patients with extensively pretreated refractory colorectal cancer metastatic to the liver
Abstract
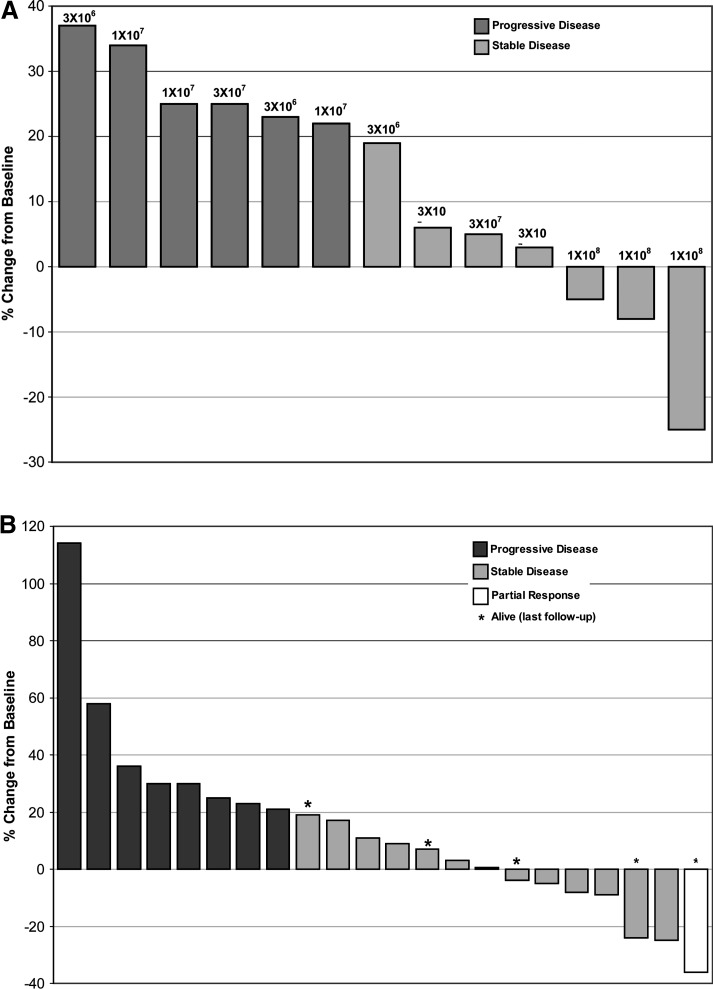
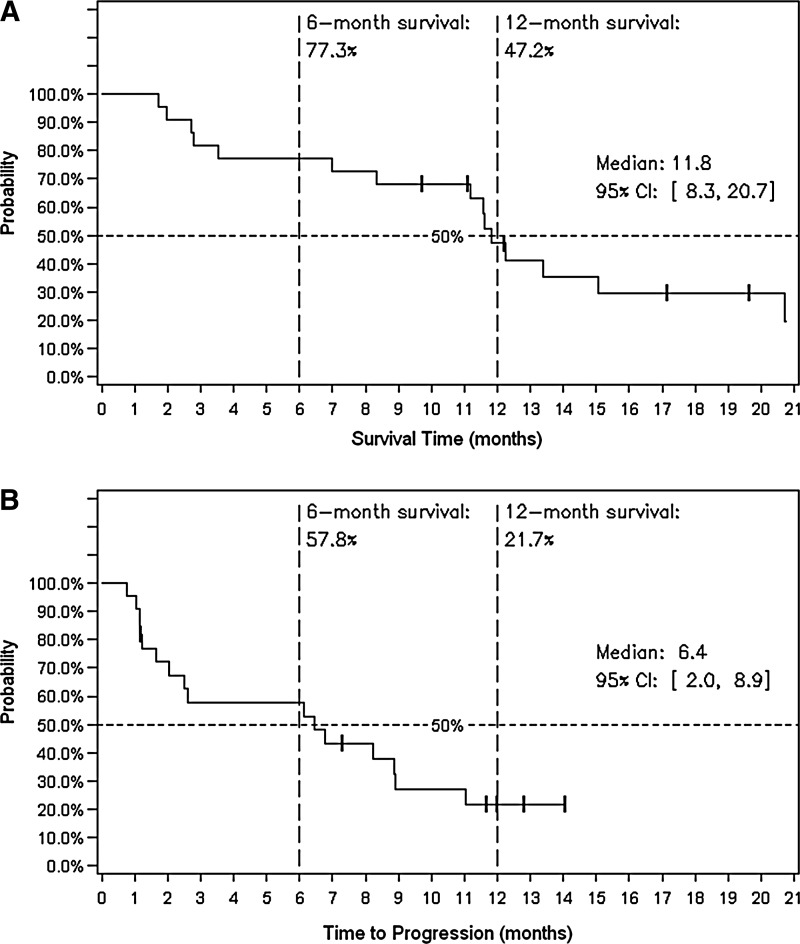
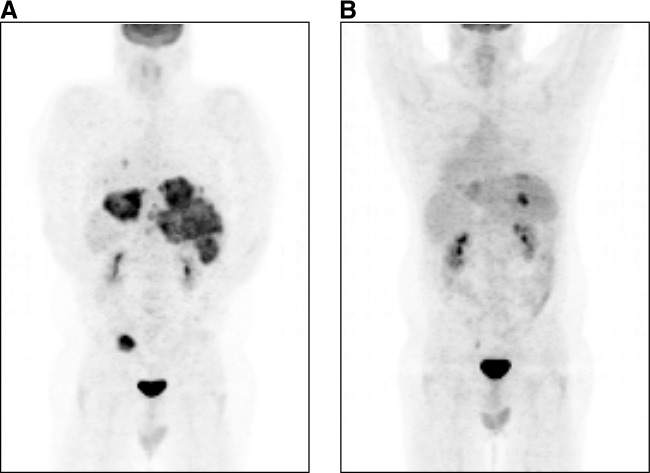
This multicenter phase I/II study evaluated the safety, pharmacokinetics, and antitumor effects of repeated doses of NV1020, a genetically engineered oncolytic herpes simplex virus, in patients with advanced metastatic colorectal cancer (mCRC). Patients with liver-dominant mCRC received four fixed NV1020 doses via weekly hepatic artery infusion, followed by two or more cycles of conventional chemotherapy. Phase I included cohorts receiving 3 × 10(6), 1 × 10(7), 3 × 10(7), and 1 × 10(8) plaque-forming units (PFU)/dose to determine the optimal biological dose (OBD) for phase II. Blind independent computed tomography scan review was based on RECIST (response evaluation criteria in solid tumors) to assess hepatic tumor response. Phase I and II enrolled 13 and 19 patients, respectively. Patients experienced transient mild-moderate febrile reactions after each NV1020 infusion. Grade 3/4 virus-related toxicity was limited to transient lymphopenia in two patients. NV1020 shedding was not detected. Simultaneous cytokine and grade 1 coagulation perturbations were dose-limiting at 1 × 10(8) PFU/dose, considered the OBD. All 22 OBD patients had previously received 5-fluorouracil; most had received oxaliplatin or irinotecan (50% had both), many with at least one targeted agent. After NV1020 administration, 50% showed stable disease. The best overall tumor control rate after chemotherapy was 68% (1 partial response, 14 stable disease); this did not correlate with baseline variables or chemotherapy. Median time to progression was 6.4 months (95% confidence interval: 2, 8.9); median overall survival was 11.8 months (95% confidence interval: 8.3, 20.7). One-year survival was 47.2%. We conclude that NV1020 stabilizes liver metastases with minimal toxicity in mCRC. It may resensitize metastases to salvage chemotherapy and extend overall survival. A randomized phase II/III trial now appears justified.
Figures
References
-
- Akiihiro N. Chenhong L. Azhang L. Ushjima Y. Ishida D. Kamakura M. Fujimoto Y.F. Goshima F. Kikkawa F. Nishiyama Y. Non-engineered, naturally oncolytic herpes simplex virus HSV1 HF-10: Applications for gene therapy. Curr. Gene Ther. 2008;8:208–221. - PubMed
-
- Biasco G. Derenzini E. Grazi G.L. Ercolani G. Ravaioli M. Pantaleo M.A. Brandi G. Treatment of hepatic metastases from colorectal cancer: Many doubts, some certainties. Cancer Treatment Rev. 2005;32:214–228. - PubMed
-
- Cadoz M. Micoud M. Seigneurin J.M. Mallaret M.R. Baccard C. Morand P. Phase 1 trial of R7020: A live attenuated recombinant herpes simplex (HSV) candidate vaccine. Paper presented at the 32nd Interscience Conference on Antimicrobial Agents and Chemotherapy; Anaheim, CA: 1992. Oct 11–14, 1992.
-
- Capdevila J. Ramos F. Macarulla T. Elez E. Tabernero J. The role of salvage treatment in advanced colorectal cancer. Crit. Rev. Oncol. Hematol. 2008;71:53–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
