

Regeneration of dental-pulp-like tissue by chemotaxis-induced cell homing
- PMID: 20486799
- PMCID: PMC2947424
- DOI: 10.1089/ten.TEA.2010.0181
Regeneration of dental-pulp-like tissue by chemotaxis-induced cell homing
Abstract
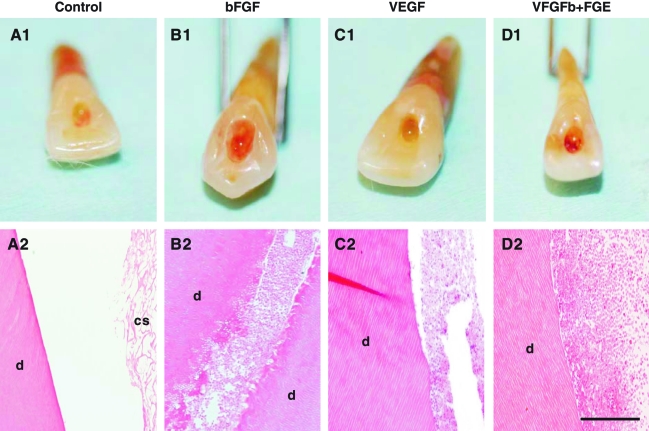
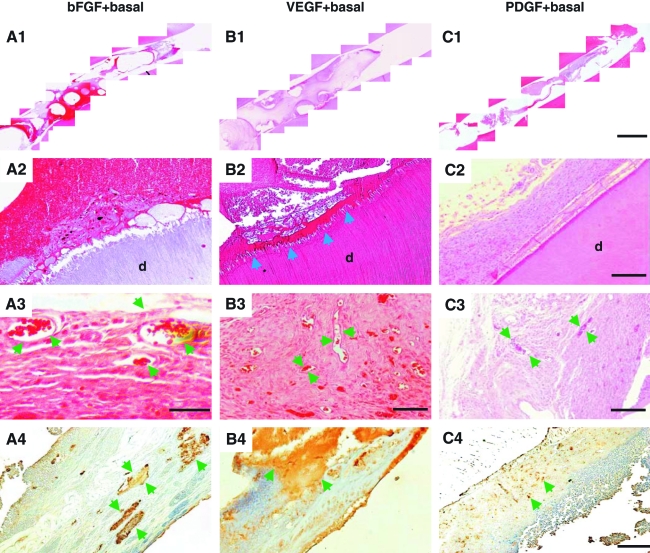
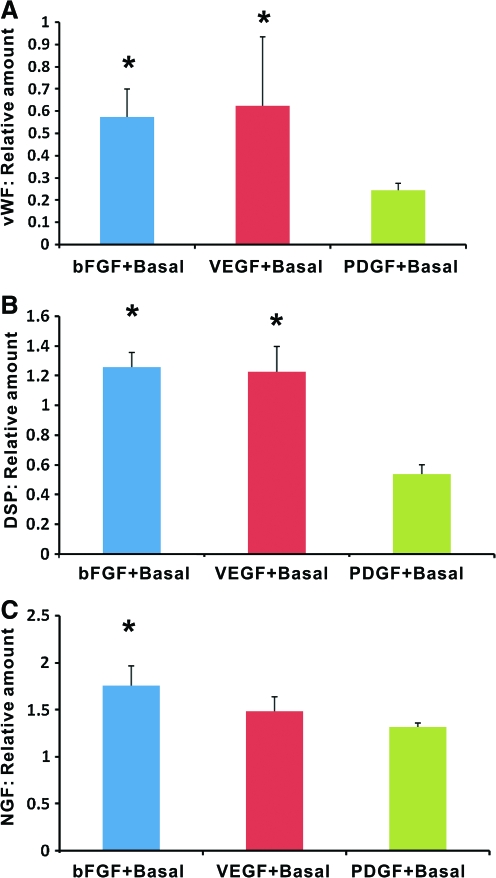
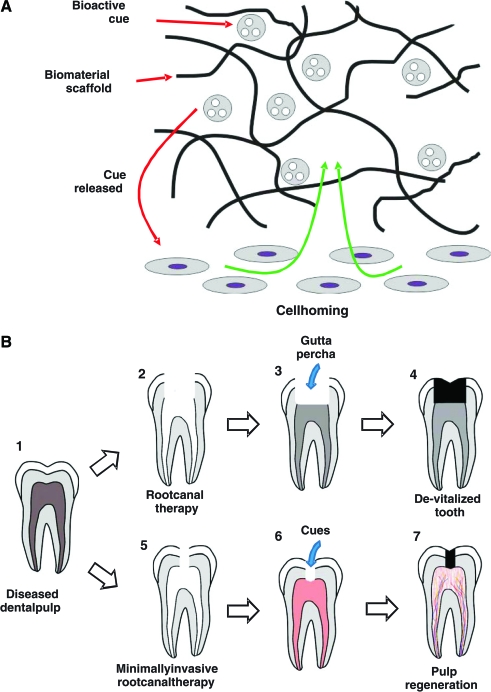
Tooth infections or injuries involving dental pulp are treated routinely by root canal therapy. Endodontically treated teeth are devitalized, susceptible to re-infections, fractures, and subsequent tooth loss. Here, we report regeneration of dental-pulp-like tissue by cell homing and without cell transplantation. Upon in vivo implantation of endodontically treated real-size, native human teeth in mouse dorsum for the tested 3 weeks, delivery of basic fibroblast growth factor and/or vascular endothelial growth factor (bFGF and/or VEGF) yielded re-cellularized and revascularized connective tissue that integrated to native dentinal wall in root canals. Further, combined delivery of bFGF, VEGF, or platelet-derived growth factor (PDGF) with a basal set of nerve growth factor (NGF) and bone morphogenetic protein-7 (BMP7) generated cellularized and vascularized tissues positive of VEGF antibody staining and apparent neo-dentin formation over the surface of native dentinal wall in some, but not all, endodontically treated teeth. Newly formed dental pulp tissue appeared dense with disconnected cells surrounded by extracellular matrix. Erythrocyte-filled blood vessels were present with endothelial-like cell lining. Reconstructed, multiple microscopic images showed complete fill of dental-pulp-like tissue in the entire root canal from root apex to pulp chamber with tissue integration to dentinal wall upon delivery of bFGF, VEGF, or PDGF with a basal set of NGF and BMP7. Quantitative ELISA showed that combinatory delivery of bFGF, VEGF, or PDGF with basal NGF and BMP7 elaborated von Willerbrand factor, dentin sialoprotein, and NGF. These findings represent the first demonstration of regenerated dental-pulp-like tissue in endodontically treated root canals of real-size, native human teeth. The present chemotaxis-based approach has potent cell homing effects for re-cellularization and revascularization in endodontically treated root canals in vivo, although in an ectopic model. Regeneration of dental pulp by cell homing, rather than cell delivery, may accelerate clinical translation.
Figures
References
-
- Ten Cate A.R. Dentin and pulp. In: Ten Cate A.R., editor. Oral Histology. London: Mosby; 1998. pp. 246–278.
-
- Ingle J.I. Bakland L.K. Structure and function of the dentin-pulp complex. In: Ingle J.I., editor; Bakland L.K., editor. Endodontics. Hamilton, Ontario, London: BC Decker, Inc.; 2002. pp. 121–143.
-
- Dammaschke T. Steven D. Kaup M. Ott K.H. Long-term survival of root-canal-treated teeth: a retrospective study over 10 years. J Endod. 2003;29:638. - PubMed
-
- Andreasen J.O. Farik B. Munksgaard E.C. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent Traumatol. 2002;18:134. - PubMed
-
- Caplan D.J. Cai J. Yin G. White B.A. Root canal filled versus non-root canal filled teeth: a retrospective comparison of survival times. J Public Health Dent. 2005;65:90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
