

Retention of HIV-infected and HIV-exposed children in a comprehensive HIV clinical care programme in Western Kenya
- PMID: 20487430
- PMCID: PMC2929358
- DOI: 10.1111/j.1365-3156.2010.02539.x
Retention of HIV-infected and HIV-exposed children in a comprehensive HIV clinical care programme in Western Kenya
Abstract
Background: To describe incidence rates (IR) and risk factors for loss-to-follow-up (LTFU) among HIV-infected and HIV-exposed children in a large HIV treatment programme in Western Kenya.
Methods: The USAID-AMPATH Partnership has enrolled >100,000 patients (20% children) at 23 clinic sites throughout western Kenya. LTFU is defined as being absent from the clinic for >3 months if on combination antiretroviral treatment (cART) and >6 months if not. Included in this analysis were children aged <14 years, HIV exposed or infected at enrollment, and enrolled between April 2002 and March 2009. The IR for LTFU are presented per 100 child-years (CY) of follow-up. Proportional hazards models with time-independent and time-dependent covariates were used to model factors associated with LTFU. Weight for height Z-scores were calculated using EpiInfo, with severe malnutrition being defined as a Z-score <or=-3.0. Immune suppression was defined as per WHO age-specific categories.
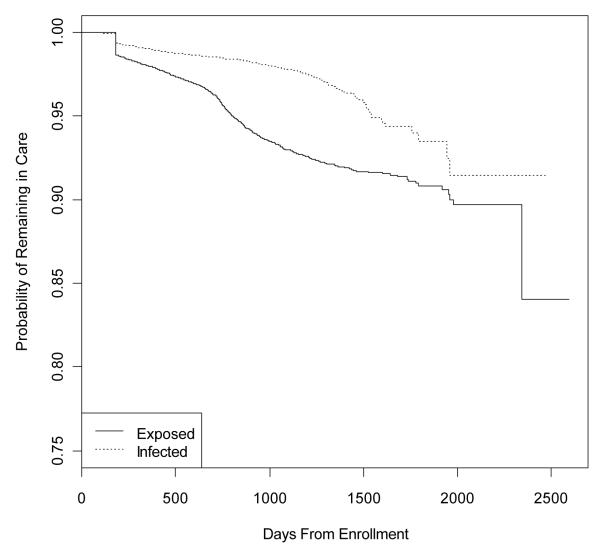
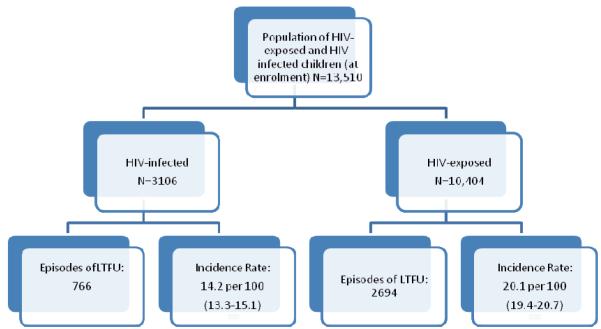
Results: There were 13,510 children eligible for analysis, comprising 3106 children who at enrollment were HIV infected and 10,404 children who were HIV exposed. The overall IR of LTFU was 18.4 (17.8-18.9) per 100 CY. Among HIV-infected children, 15.2 (13.8-16.7) and 14.1 (13.1-15.8) per 100 CY became LTFU, pre- and post-cART initiation, respectively. The only independent risk factor for becoming LTFU among the HIV-infected children was severe immune suppression (AHR: 2.17, 95% CI: 1.51-3.12). Among the HIV-exposed children, 20.1 per 100 (19.4-20.7) became LTFU. Independent risk factors for LTFU among them were being severely low weight for height (AHR: 1.69, 95% CI: 1.25-2.28), being orphaned at enrollment (AHR: 1.57, 95% CI: 1.23-1.64), being CDC Class B or C (AHR: 1.41, 95% CI: 1.14-1.74), and having received cART (AHR: 1.56, 95% CI: 1.23-1.99). Protective against becoming LTFU among the HIV exposed were testing HIV positive (AHR: 0.26, 95% CI: 0.21-0.32), older age (AHR: 0.90, 95% CI: 0.85-0.96), enrolling in later time periods, and receiving food supplementation (AHR: 0.58, 95% CI: 0.32-1.04).
Conclusions: There is a high rate of LTFU among these highly vulnerable children, particularly among the HIV exposed. These data suggest that HIV-infected and HIV-exposed children are at especially high risk for LTFU if they are sick or malnourished.
Figures
References
-
- Moatti JP, I ND, Hammer SM, et al. Antiretroviral treatment for HIV infection in developing countries: an attainable new paradigm. Nature Medicine. 2003;9(12):1449–1452. - PubMed
-
- World Health Organization . In: Towards Universal Access: Scaling up priority HIV/AIDS interventions in the health sector. W.H. Organization, editor. World Health Organization; Geneva: 2008.
-
- UNAIDS . Report on the Global AIDS Epidemic. Joint United Nations Program on HIV/AIDS; Geneva: 2008.
-
- Low risk of death, but substantial program attrition, in pediatric HIV treatment cohorts in Sub-Saharan Africa. J Acquir Immune Defic Syndr. 2008;49(5):523–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
