

Septopreoptic holoprosencephaly: a mild subtype associated with midline craniofacial anomalies
- PMID: 20488907
- PMCID: PMC7965016
- DOI: 10.3174/ajnr.A2123
Septopreoptic holoprosencephaly: a mild subtype associated with midline craniofacial anomalies
Abstract
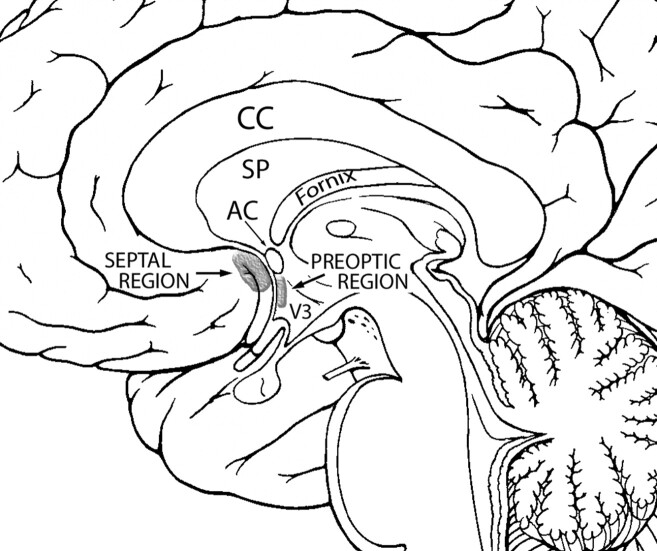
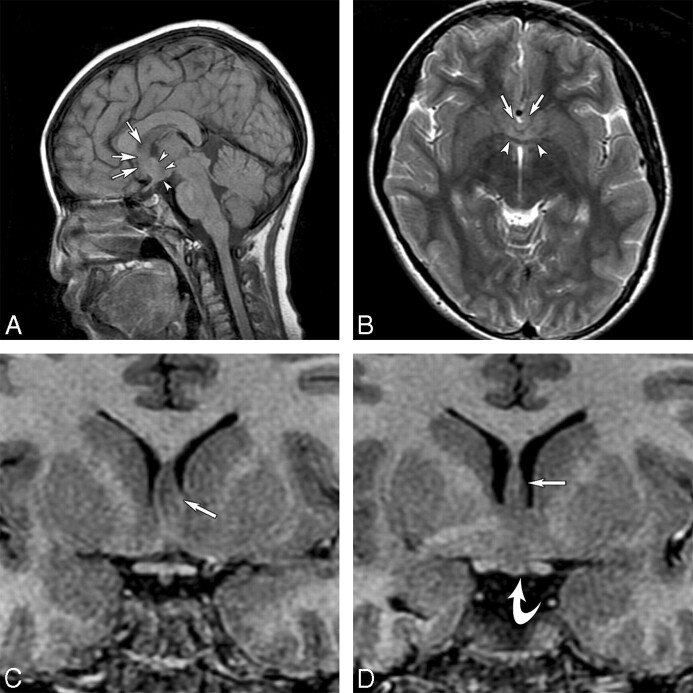
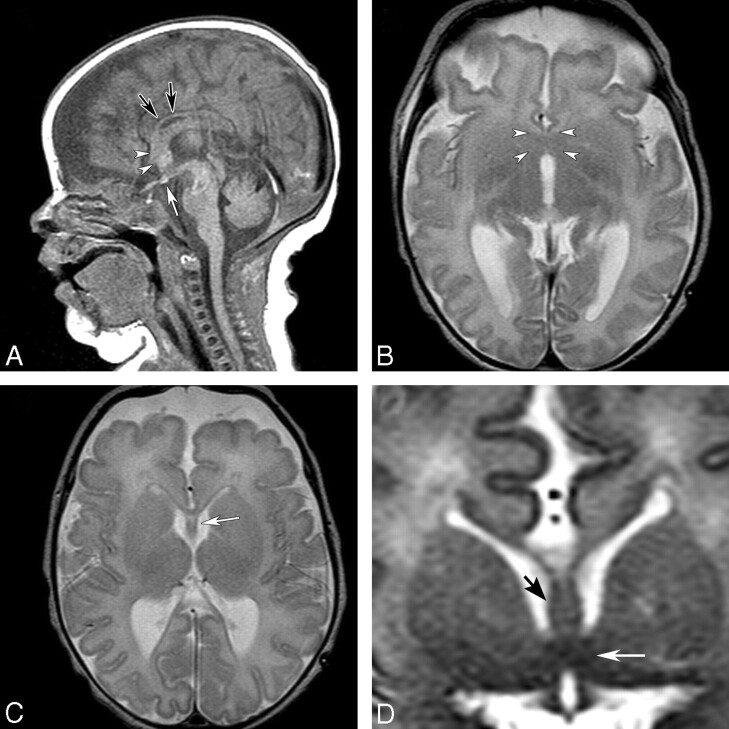
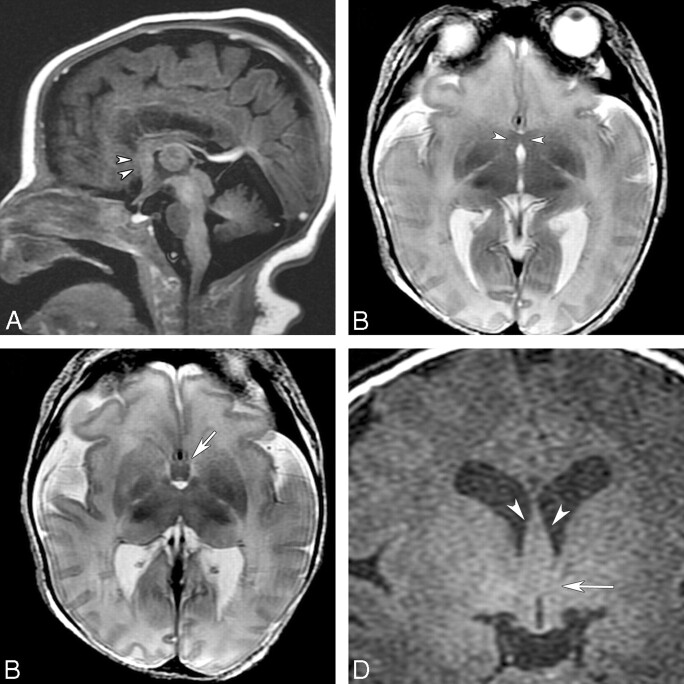
HPE is a congenital brain malformation characterized by failure of the prosencephalon to divide into 2 hemispheres. We have identified 7 patients who have a mild subtype of HPE in which the midline fusion was restricted to the septal region or preoptic region of the telencephalon. This subtype, which we call septopreoptic HPE, falls in the spectrum of lobar HPE, but lacks significant frontal neocortical fusion seen in lobar HPE. Other imaging characteristics include thickened or dysplastic fornix, absent or hypoplastic anterior CC, and single unpaired ACA. The SP was fully formed in 4, partially formed in 2, and absent in 1. Mild midline craniofacial malformation, such as SMMCI and CNPAS were found in 86% and 71%, respectively. Patients outside of infancy often manifested language delay, learning disabilities, or behavioral disturbances, while motor function was relatively spared.
Figures
References
-
- Golden JA. Towards a greater understanding of the pathogenesis of holoprosencephaly. Brain Dev 1999; 21: 513– 21 - PubMed
-
- DeMyer W. Holoprosencephaly (cyclopia-arrhinencephaly). In: Vinken PJ, Bruyn GW, Klawans HL.eds. Handbook of Clinical Neurology. 6th ed. Amsterdam, the Netherlands: Elsevier Science Publishers; 1987: 225– 44
-
- Lewis AJ, Simon EM, Barkovich AJ, et al. Middle interhemispheric variant of holoprosencephaly: a distinct cliniconeuroradiologic subtype. Neurology 2002; 59: 1860– 65 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous