

Canine spontaneous glioma: a translational model system for convection-enhanced delivery
- PMID: 20488958
- PMCID: PMC2940703
- DOI: 10.1093/neuonc/noq046
Canine spontaneous glioma: a translational model system for convection-enhanced delivery
Abstract
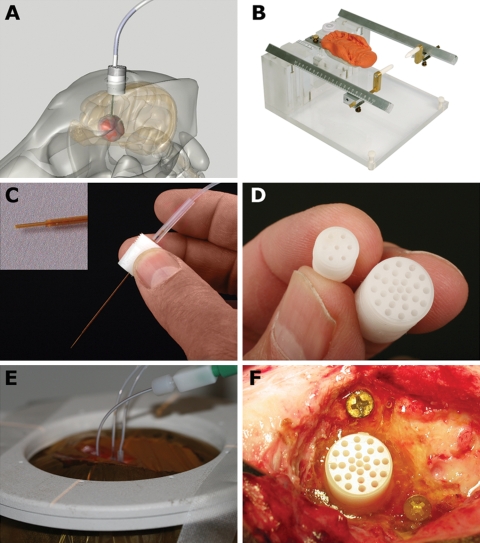
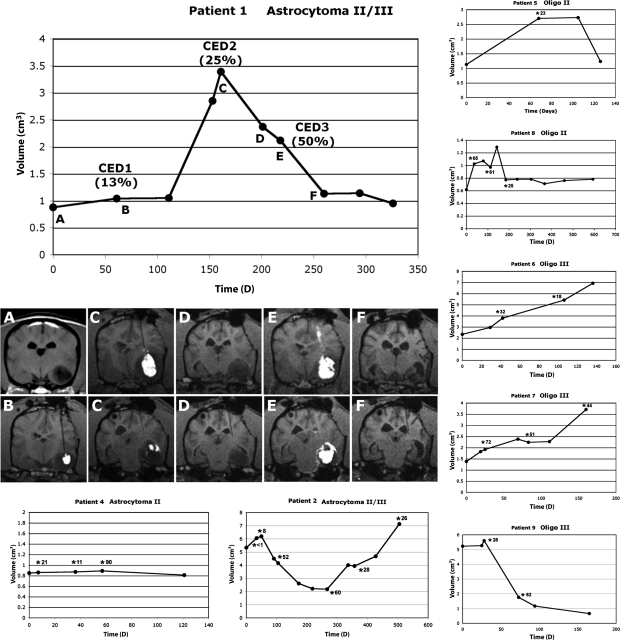
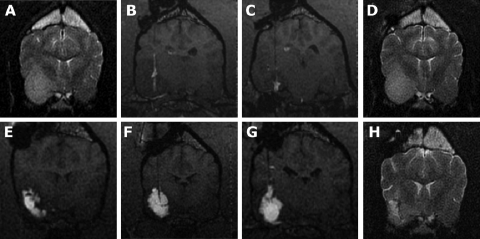
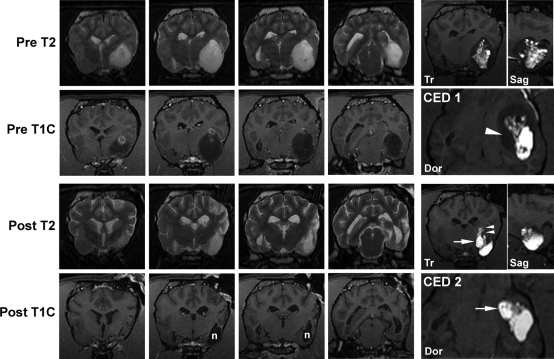
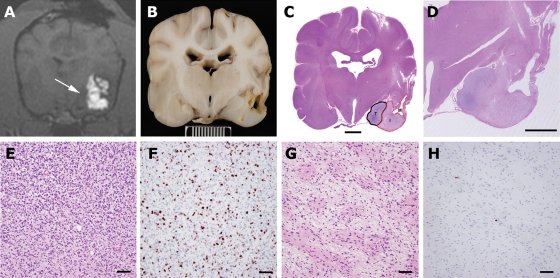
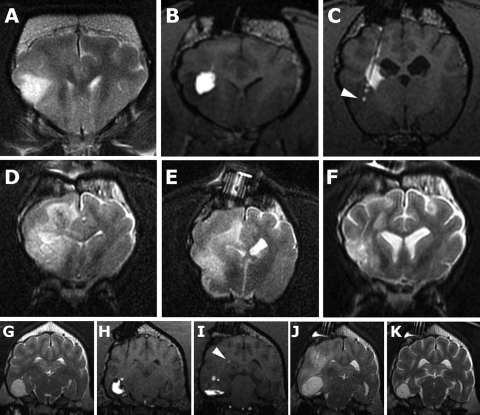
Canine spontaneous intracranial tumors bear striking similarities to their human tumor counterparts and have the potential to provide a large animal model system for more realistic validation of novel therapies typically developed in small rodent models. We used spontaneously occurring canine gliomas to investigate the use of convection-enhanced delivery (CED) of liposomal nanoparticles, containing topoisomerase inhibitor CPT-11. To facilitate visualization of intratumoral infusions by real-time magnetic resonance imaging (MRI), we included identically formulated liposomes loaded with Gadoteridol. Real-time MRI defined distribution of infusate within both tumor and normal brain tissues. The most important limiting factor for volume of distribution within tumor tissue was the leakage of infusate into ventricular or subarachnoid spaces. Decreased tumor volume, tumor necrosis, and modulation of tumor phenotype correlated with volume of distribution of infusate (Vd), infusion location, and leakage as determined by real-time MRI and histopathology. This study demonstrates the potential for canine spontaneous gliomas as a model system for the validation and development of novel therapeutic strategies for human brain tumors. Data obtained from infusions monitored in real time in a large, spontaneous tumor may provide information, allowing more accurate prediction and optimization of infusion parameters. Variability in Vd between tumors strongly suggests that real-time imaging should be an essential component of CED therapeutic trials to allow minimization of inappropriate infusions and accurate assessment of clinical outcomes.
Figures
Similar articles
-
A phase I study of convection-enhanced delivery (CED) of liposomal-irinotecan using real-time magnetic resonance imaging in patients with recurrent high-grade glioma.J Neurooncol. 2025 Mar;172(1):219-227. doi: 10.1007/s11060-024-04904-y. Epub 2025 Jan 6. J Neurooncol. 2025. PMID: 39760796 Free PMC article. Clinical Trial.
-
Canine model of convection-enhanced delivery of liposomes containing CPT-11 monitored with real-time magnetic resonance imaging: laboratory investigation.J Neurosurg. 2008 May;108(5):989-98. doi: 10.3171/JNS/2008/108/5/0989. J Neurosurg. 2008. PMID: 18447717
-
Effects of convection-enhanced delivery of bevacizumab on survival of glioma-bearing animals.Neurosurg Focus. 2015 Mar;38(3):E8. doi: 10.3171/2015.1.FOCUS14743. Neurosurg Focus. 2015. PMID: 25727230
-
Real-time imaging and quantification of brain delivery of liposomes.Pharm Res. 2006 Nov;23(11):2493-504. doi: 10.1007/s11095-006-9103-5. Epub 2006 Sep 14. Pharm Res. 2006. PMID: 16972184 Review.
-
Convection enhanced drug delivery of novel therapeutic agents to malignant brain tumors.Curr Drug Deliv. 2007 Apr;4(2):169-80. doi: 10.2174/156720107780362302. Curr Drug Deliv. 2007. PMID: 17456036 Review.
Cited by
-
Chemotherapy for the treatment of intracranial glioma in dogs.Front Vet Sci. 2023 Oct 31;10:1273122. doi: 10.3389/fvets.2023.1273122. eCollection 2023. Front Vet Sci. 2023. PMID: 38026627 Free PMC article. Review.
-
Toward intracellular targeted delivery of cancer therapeutics: progress and clinical outlook for brain tumor therapy.BioDrugs. 2012 Aug 1;26(4):235-44. doi: 10.2165/11631600-000000000-00000. BioDrugs. 2012. PMID: 22671766 Free PMC article.
-
Comparison of linear and volumetric criteria for the determination of therapeutic response in dogs with intracranial gliomas.J Vet Intern Med. 2022 May;36(3):1066-1074. doi: 10.1111/jvim.16406. Epub 2022 Mar 11. J Vet Intern Med. 2022. PMID: 35274379 Free PMC article.
-
New agents for targeting of IL-13RA2 expressed in primary human and canine brain tumors.PLoS One. 2013 Oct 16;8(10):e77719. doi: 10.1371/journal.pone.0077719. eCollection 2013. PLoS One. 2013. PMID: 24147065 Free PMC article.
-
Epidermal growth factor receptor activity is elevated in glioma cancer stem cells and is required to maintain chemotherapy and radiation resistance.Oncotarget. 2017 Aug 3;8(42):72494-72512. doi: 10.18632/oncotarget.19868. eCollection 2017 Sep 22. Oncotarget. 2017. PMID: 29069805 Free PMC article.
References
-
- Fomchenko EI, Holland EC. Mouse models of brain tumors and their applications in preclinical trials. Clin Cancer Res. 2006;12:5288–5297. doi:10.1158/1078-0432.CCR-06-0438. - DOI - PubMed
-
- Branle F, Lefranc F, Camby I, et al. Evaluation of the efficiency of chemotherapy in in vivo orthotopic models of human glioma cells with and without 1p19q deletions and in C6 rat orthotopic allografts serving for the evaluation of surgery combined with chemotherapy. Cancer. 2002;95:641–655. doi:10.1002/cncr.10710. - DOI - PubMed
-
- Vail DM, MacEwen EG. Spontaneously occurring tumors of companion animals as models for human cancer. Cancer Invest. 2000;18:781–792. doi:10.3109/07357900009012210. - DOI - PubMed
-
- Koestner A, Bilzer T, Fatzer R, Schulman FY, Summers BA, Van Winkle TJ. Histological Classification of Tumors of the Nervous System of Domestic Animals. 2nd ed. vol. 5. Washington, D.C: The Armed Forces Institute of Pathology; 1999.
-
- Paoloni M, Khanna C. Translation of new cancer treatments from pet dogs to humans. Nat Rev Cancer. 2008;8:147–156. doi:10.1038/nrc2273. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
