

Review
doi: 10.2214/AJR.09.3736.
Soft-tissue masses and masslike conditions: what does CT add to diagnosis and management?
Affiliations
- PMID: 20489097
- PMCID: PMC2884142
- DOI: 10.2214/AJR.09.3736
Item in Clipboard
Review
Soft-tissue masses and masslike conditions: what does CT add to diagnosis and management?
AJR Am J Roentgenol.
2010 Jun.
Abstract
Objective: Although MRI is the technique of choice for evaluating most soft-tissue masses, CT often provides valuable complementary information. Specifically, there are distinguishing CT characteristics that can suggest a specific diagnosis, including the lesion's mineralization pattern, density, pattern of adjacent bone involvement, and degree and pattern of vascularity.
Conclusion: This article provides an overview of the CT evaluation of soft-tissue masses, emphasizing a differential diagnosis based on these CT features.
Figures
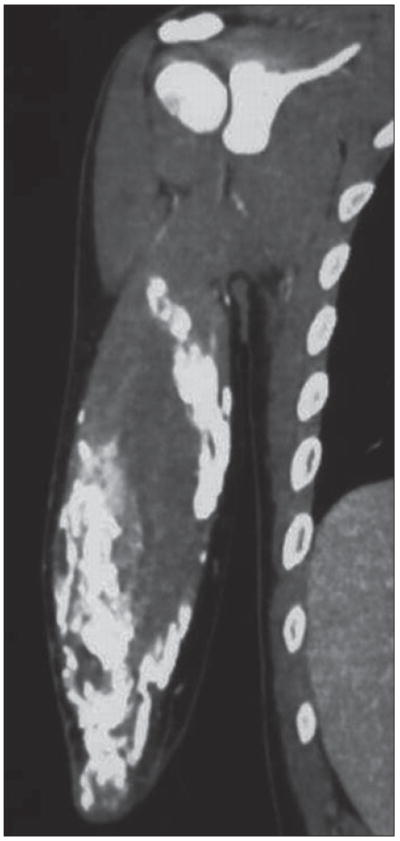
58-year-old man with dermatomyositis. Coronal CT multiplanar reconstruction shows sheetlike calcifications around biceps brachii muscle, appearance termed calcinosis universalis. Such subcutaneous and soft-tissue calcifications can be seen in other connective tissue disorders, notably scleroderma.
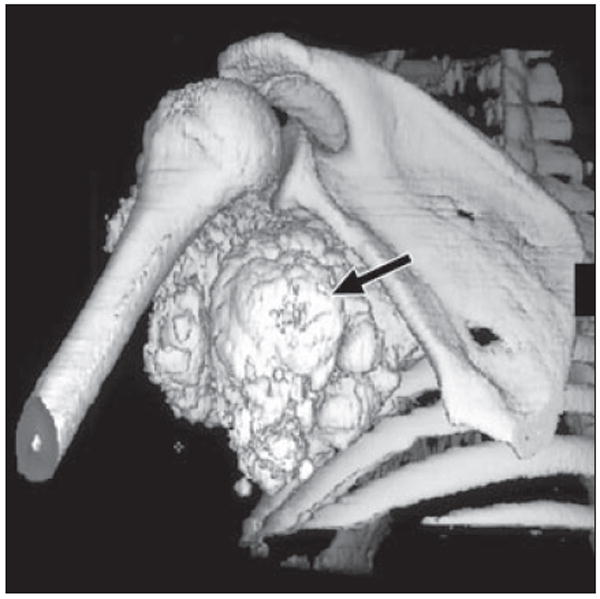
39-year-old man with metastatic calcification in end-stage renal disease due to glomerulonephritis. Patient had elevated serum calcium and presented with soft-tissue mass (arrow) in his left axillary recess that was encasing his brachial plexus, resulting in arm pain and weakness. Shaded surface display image from axial oblique perspective of left shoulder depicts relationship of mass to adjacent shoulder girdle, useful for surgical planning.

69-year-old man with gout. Patient presented with swelling and pain in left arm. Coronal volume-rendered CT image shows soft tissue mass posterior to olecranon with amorphous calcification (arrow), consistent with soft-tissue tophus. Tophaceous gout typically presents as juxtaarticular lobulated soft tissue mass, occasionally with calcifications, and has predilection for olecranon and prepatellar regions. Incidental cardiac pacemaker is seen in upper left chest.
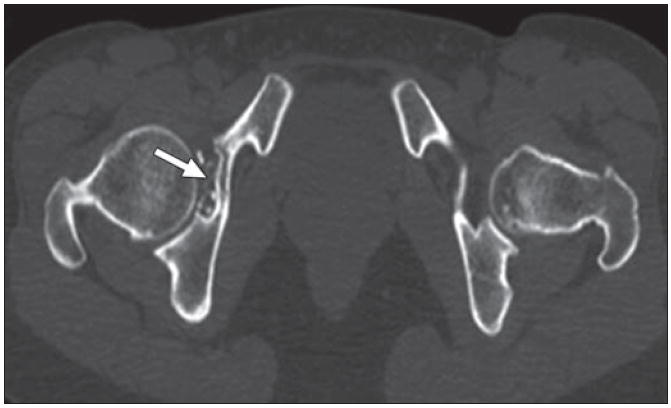
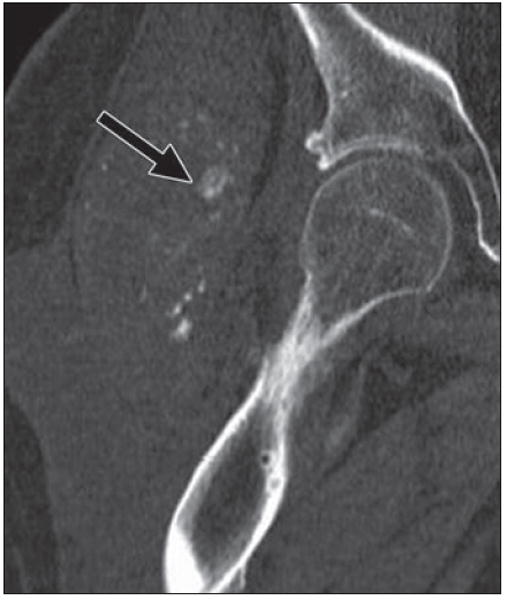
37-year-old woman with synovial chondromatosis. Intraarticular calcified bodies in right hip are seen on axial CT. Note associated cortical scalloping of acetabulum (arrow), all features of synovial chondromatosis.
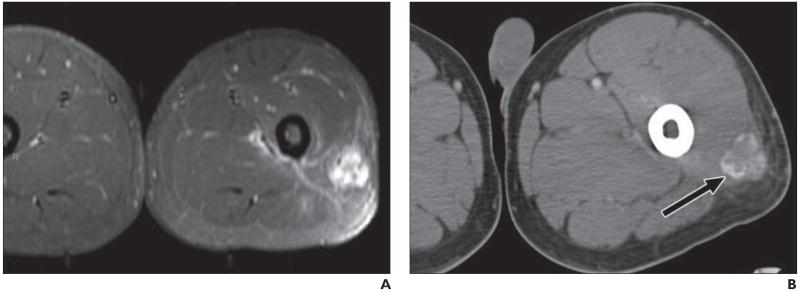
21-year-old man presenting with several-week-long history of painful mass in his left thigh that was “growing by day.” Patient denied history of trauma, and radiography results were negative. A, MRI shows nonspecific soft-tissue mass in posterolateral thigh with diffuse enhancement and surrounding edema, as seen on fat-saturated axial T1-weighted image obtained after administration of gadolinium contrast agent. B, Follow-up CT suggests final diagnosis of heterotopic ossification (myositis ossificans) by revealing characteristic peripheral zone (“eggshell”) of ossification (arrow). Patients with myositis ossificans are frequently young patients without known history of trauma, and thigh is most common location. Rim of mineralization is typically seen on CT by 4–6 weeks and is important discriminator from soft-tissue tumor.
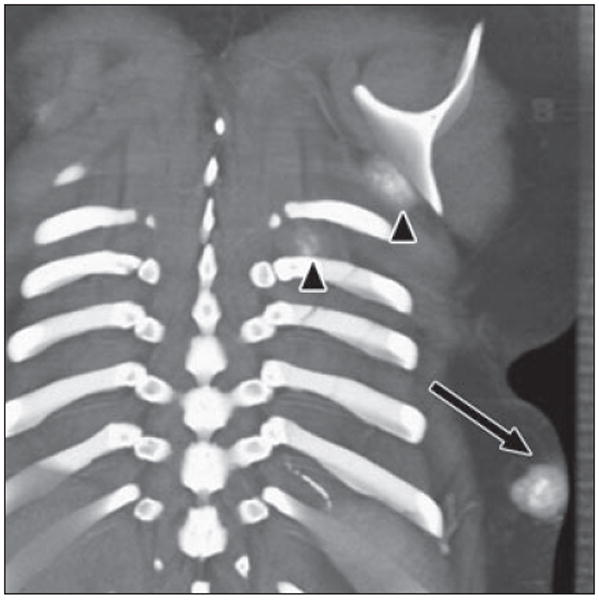
17-year-old girl with history of osteosarcoma of left fibula. Coronal volume-rendered image reveals mass within subcutaneous tissues of posterior left lower chest with cloudlike calcification (arrow), consistent with soft-tissue metastasis due to osteosarcoma. Two smaller masses are seen inferior to left scapula and between left ribs (arrowheads). Fluffy ossification in soft tissues with central hyperdense ossification is characteristic of osteoid matrix.

46-year-old man with slowly growing chest mass over 2 years. Axial CT image on bone windows shows soft-tissue mass arising at anterior costochondral junction, with punctate and arclike patterns of calcification and underlying osseous involvement. Radiologic and histologic features were compatible with intermediate grade chondrosarcoma.
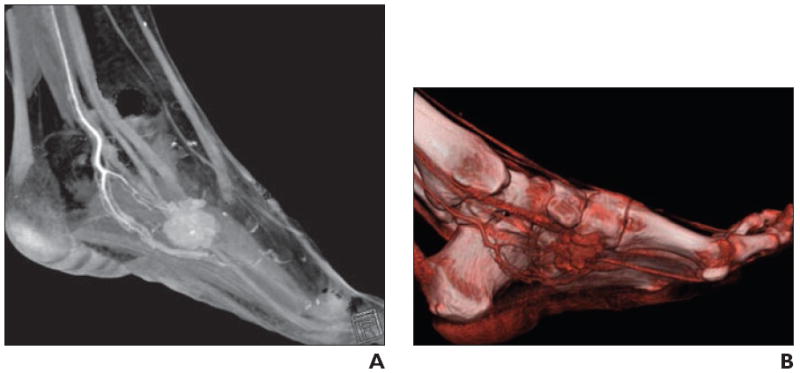
34-year-old woman with palpable soft tissue mass in foot. A, Volume-rendered 3D CT image in sagittal plane shows vascular mass, as evidenced by homogeneous contrast enhancement, associated with internal calcification. B, Shading to optimize visualization of vasculature better delineates arterial supply, which is useful for operative planning. Constellation of findings suggests synovial sarcoma.
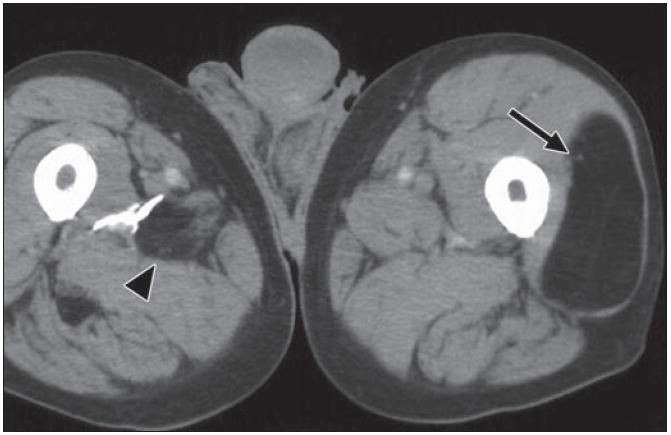
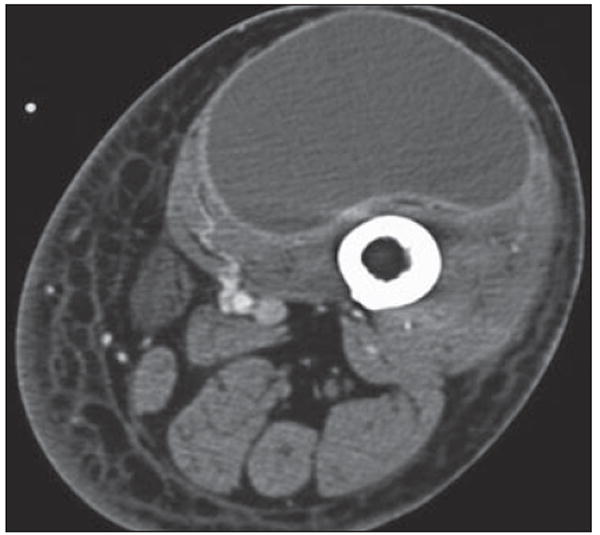
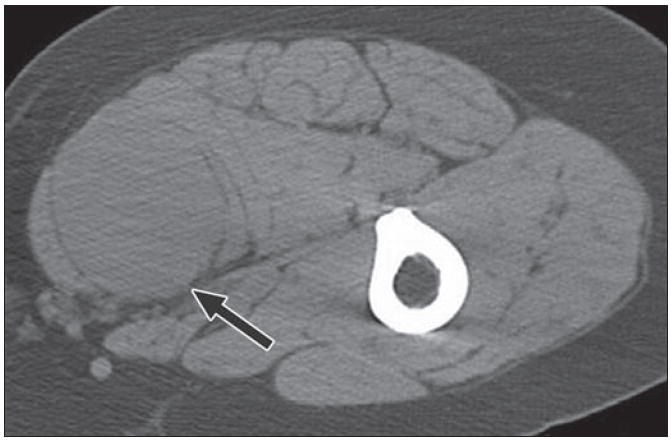
82-year-old man who noticed new “lump” on his leg. Axial CT depicts well-defined fat density mass within his left vastus lateralis muscle, with few very thin internal soft tissue septations (arrow). Finding is consistent with benign intramuscular lipoma. Incidentally, within posterior musculature of right thigh another smaller fat density mass (arrowhead) with internal stranding is present, probably due to interdigitating muscle fibers through lipoma.
49-year-old woman who presented with enlarging mass in right posterior thigh. Axial CT shows predominantly fatty mass with areas of internal soft-tissue stranding and some nodularity (arrows). Surgery revealed well-differentiated liposarcoma or atypical lipomatous tumor. This is low-grade tumor that does not tend to metastasize but can recur locally after excision.

70-year-old man with continued swelling of his left leg, originally thought to be due to lymphedema. Coronal multiplanar reconstruction CT reveals large predominantly fat density lesion infiltrating and replacing posterior and medial musculature of thigh. Mass contains multiple areas of nodularity, as well as portions encapsulated by thick and irregular septations (arrow) superiorly, consistent with higher grade liposarcoma.
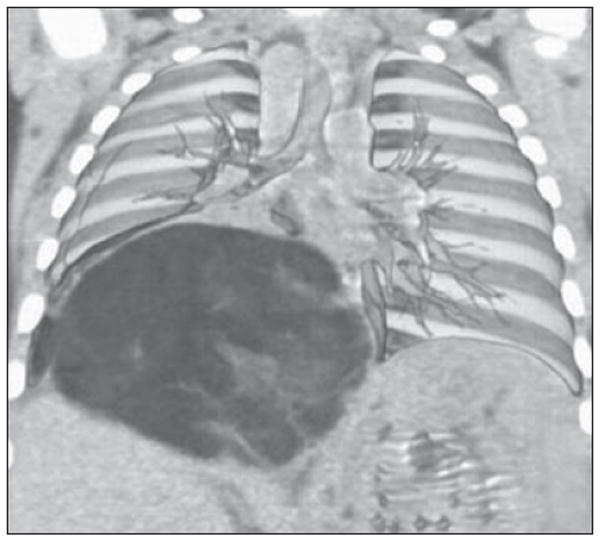
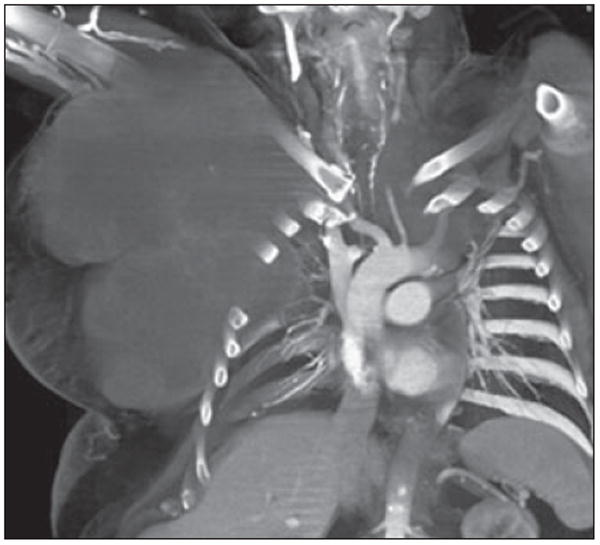
6-month-old boy with cough who was found to have large soft-tissue mass within chest on radiograph. Coronal volume-rendered image shows how mass displaces liver inferiorly and splays overlying pulmonary vasculature. Pathologic analysis revealed mass to be lipoblastoma, which is rare tumor of infancy and may radiographically resemble liposarcoma. Liposarcomas are extremely rare in children.
72-year-old man with swelling in left groin and thigh after thoracic aneurysm repair. Axial CT shows diffuse swelling of left lower extremity with cystic mass surrounded by thin rim of contrast enhancement within quadriceps. Although this appearance is consistent with lymphangioma, seroma, or abscess, this was lymphocele at resection.
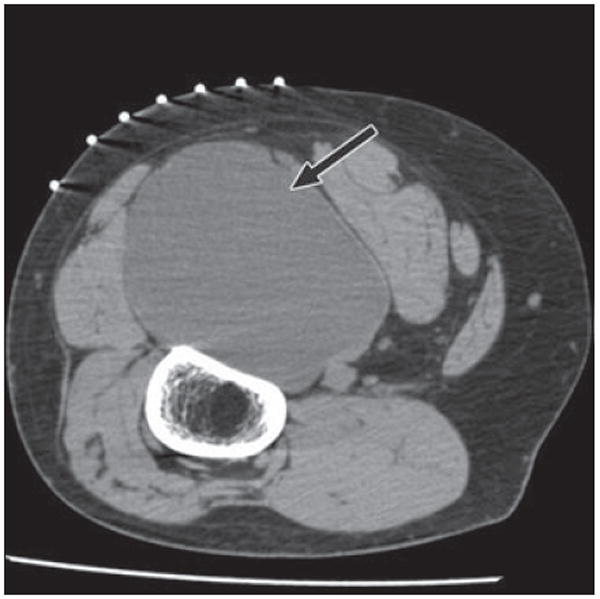
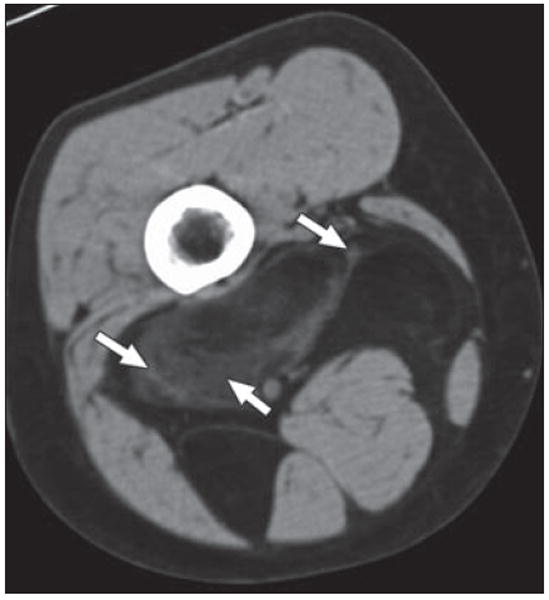
46-year-old man with mass in posterior left thigh. Axial CT image with patient in prone position for biopsy shows large cystic mass (arrow) posterior to femur, splaying hamstrings. Pathologic analysis revealed myxoid liposarcoma, which may have soft-tissue or pseudocystic appearance, mimicking intramuscular myxoma. Myxoid as well as pleomorphic liposarcomas may show minimal fat, and approximately 20% of lesions have completely cystic appearance. A cystic-appearing tumor within soft tissues of extremities thus always requires biopsy.
35-year-old woman diagnosed with Gardener syndrome, in setting of diffuse colonic polyposis, developed firm mass in her anterior abdominal wall. Axial CT image shows mass (arrow) in left rectus muscle, of similar attenuation to surrounding muscle, compatible with desmoid.
61-year-old woman with 2-year history of right thigh mass. Axial CT with patient prone shows intermediate density mass (arrow) splaying gracilis and adductor longus in posteromedial thigh. Fibrous masses within soft tissues usually have nonspecific appearance and biopsy is required for further characterization. This was solitary fibrous tumor.
43-year-old man, quadriplegic after motorcycle accident, who had right hip pain for 2 months. Coronal multiplanar reconstruction CT image shows large masses of mixed attenuation lateral to right hip, with erosion of adjacent greater trochanter and shaft of right femur. There are scattered flocculent calcifications (arrow) within masses. This process involved both hips and was consistent with amyloid at biopsy. Benign soft-tissue masses affect adjacent bone commonly with pressure erosion or scalloping.
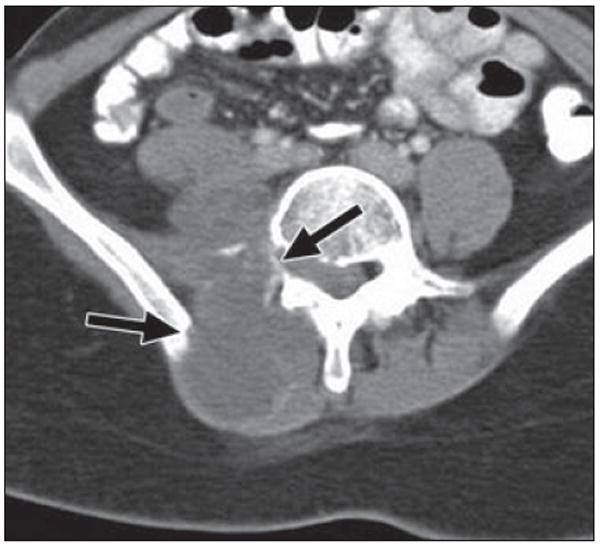
22-year-old woman with history of Wilms tumor (at age 6 years), with right-sided back pain and shooting pain down her right leg for 2 months. Axial CT image shows large heterogeneous mass within right paraspinal musculature invading right iliopsoas muscle and aggressive destruction of bone (arrows) involving right transverse process of vertebral body and right iliac ring. Pathologic lesion was consistent with high-grade postradiation sarcoma.
56-year-old man with metastatic chordoma, presenting as enormous soft-tissue mass projecting from right anterior chest wall. Primary tumor arose in posterior mediastinum. Coronal volume-rendered image reveals large low-density soft-tissue mass growing around and splaying ribs and protruding into pleural space without destruction of adjacent bone. Although chordomas are histologically low-grade neoplasms, they may have extensive local invasion and high rate of recurrence.

31-year-old man with arteriovenous malformation involving radial aspect of right wrist. Volume-rendered 3D CT image allows global appreciation of extent of involvement, which is particularly useful for treatment planning.
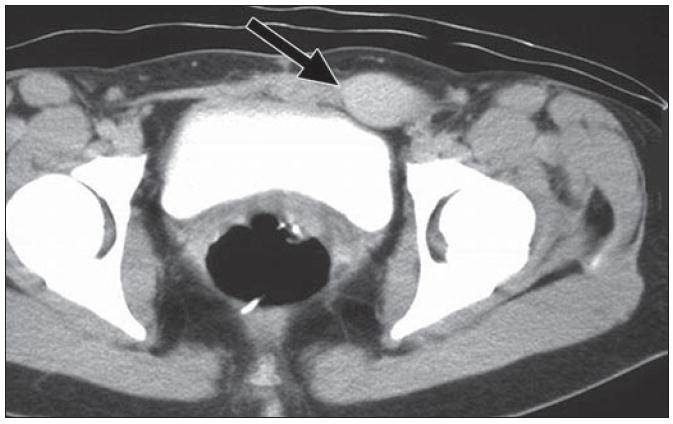
24-year-old man who was born with small cutaneous pigmented patch over his anterior abdominal wall and slowly developed mass subjacent to this site. Axial CT shows mixed attenuation mass arising from left rectus muscle and protruding into anterior left pelvis. A large feeding vessel (arrow) appears to supply mass. Note also numerous low-attenuation areas coursing through mass indicative of lipid content, another CT characteristic that can be used for characterization, seen in vascular malformations. At resection, it was found to be intramuscular capillary vascular malformation.
Comment in
-
Diagnosis of soft-tissue masses.AJR Am J Roentgenol. 2011 Aug;197(2):W365. doi: 10.2214/AJR.10.5203. AJR Am J Roentgenol. 2011. PMID: 21785068 No abstract available.
References
-
- Wu JM, Montgomery E. Classification and pathology. Surg Clin North Am. 2008;88:483–520. v–vi. - PubMed
-
- Murphey MD. World Health Organization classification of bone and soft tissue tumors: modifications and implications for radiologists. Semin Musculoskelet Radiol. 2007;11:201–214. - PubMed
-
- Egund N, Ekelund L, Sako M, Persson B. CT of soft-tissue tumors. AJR. 1981;137:725–729. - PubMed
-
- Yiu-Chiu VS, Chiu LC. Complementary values of ultrasound and computed tomography in the evaluation of musculoskeletal masses. RadioGraphics. 1983;3:46–82.
-
- Soye I, Levine E, De Smet AA, Neff JR. Computed tomography in the preoperative evaluation of masses arising in or near the joints of the extremities. Radiology. 1982;143:727–732. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
