

5% dimethyl sulfoxide (DMSO) and pentastarch improves cryopreservation of cord blood cells over 10% DMSO
- PMID: 20492608
- PMCID: PMC6525963
- DOI: 10.1111/j.1537-2995.2010.02684.x
5% dimethyl sulfoxide (DMSO) and pentastarch improves cryopreservation of cord blood cells over 10% DMSO
Abstract
Background: Cell number and viability are important in cord blood (CB) transplantation. While 10% dimethyl sulfoxide (DMSO) is the standard medium, adding a starch to freezing medium is increasingly utilized as a cytoprotectant for the thawing process. Similar to hetastarch, pentastarch has the advantages of faster renal clearance and less effect on the coagulation system.
Study design and methods: We compared a lower DMSO concentration (5%) containing pentastarch with 10% DMSO and performed cell viability assay, colony-forming units (CFUs), and transplantation of CB cells in NOD/SCID IL2Rγ(null) mice.
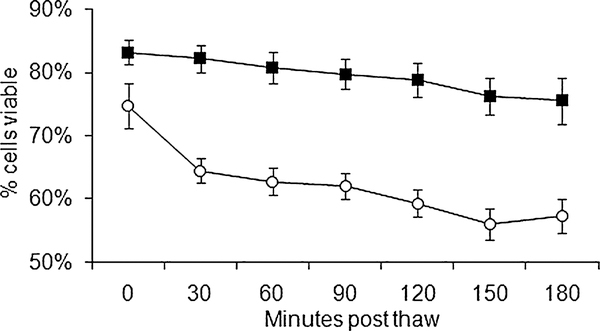
Results: CB cells in 5% DMSO/pentastarch had similar CD34+, CD3+, and CD19+ cell percentages after thawing as fresh CB cells. CB cells in 5% DMSO/pentastarch had higher viability (83.3±9.23%) than those frozen in 10% DMSO (75.3±11.0%, p<0.05). We monitored cell viability postthaw every 30 minutes. The mean loss in the first 30 minutes was less in the 5% DMSO/pentastarch group. At the end of 3 hours, the viability decreased by a mean of 7.75% for the 5% DMSO/pentastarch and 17.5% for the 10% DMSO groups. CFUs were similar between the two cryopreserved groups. Frozen CB cells engrafted equally well in IL2Rγ(null) mice compared to fresh CB cells up to 24 weeks, and CB cells frozen in 5% DMSO/pentastarch engrafted better than those in 10% DMSO.
Conclusion: Our data indicate that the lower DMSO concentration with pentastarch represents an improvement in the CB cryopreservation process and could have wider clinical application as an alternate freezing medium over 10% DMSO.
© 2010 American Association of Blood Banks.
Conflict of interest statement
CONFLICT OF INTEREST
The authors have no financial conflict of interest to declare.
Figures
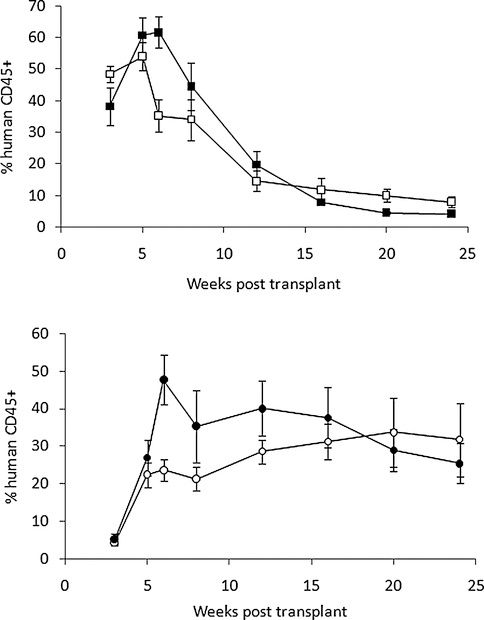

 , 2 × 107 n = 6). The mean percentages of human CD45+ cells are plotted with respect to time after transplant. When t test was used to compare the two freezing methods, 5% DMSO/pentastarch had higher human cell engraftment at 6 weeks (p = 0.027, oneway ANOVA) and 12 weeks (p = 0.042, one-way ANOVA).
, 2 × 107 n = 6). The mean percentages of human CD45+ cells are plotted with respect to time after transplant. When t test was used to compare the two freezing methods, 5% DMSO/pentastarch had higher human cell engraftment at 6 weeks (p = 0.027, oneway ANOVA) and 12 weeks (p = 0.042, one-way ANOVA).Similar articles
-
Trehalose ameliorates the cryopreservation of cord blood in a preclinical system and increases the recovery of CFUs, long-term culture-initiating cells, and nonobese diabetic-SCID repopulating cells.Transfusion. 2003 Feb;43(2):265-72. doi: 10.1046/j.1537-2995.2003.00301.x. Transfusion. 2003. PMID: 12559024
-
Polyunsaturated fatty acids confer cryoresistance on megakaryocytes generated from cord blood and also enhance megakaryocyte production from cryopreserved cord blood cells.Cytotherapy. 2012 Mar;14(3):366-80. doi: 10.3109/14653249.2011.649186. Epub 2012 Jan 17. Cytotherapy. 2012. PMID: 22250991
-
Assessing the toxic effects of DMSO on cord blood to determine exposure time limits and the optimum concentration for cryopreservation.Vox Sang. 2015 Aug;109(2):181-90. doi: 10.1111/vox.12267. Epub 2015 Apr 20. Vox Sang. 2015. PMID: 25899864
-
A strategy for processing of peripheral blood stem cells utilizing the small volume collection chamber and cryopreservation without a rate controller using pentastarch.J Hematother. 1993 Winter;2(4):525-8. doi: 10.1089/scd.1.1993.2.525. J Hematother. 1993. PMID: 7522111 Review.
-
Impact of lower concentrations of dimethyl sulfoxide on cryopreservation of autologous hematopoietic stem cells: a systematic review and meta-analysis of controlled clinical studies.Cytotherapy. 2024 May;26(5):482-489. doi: 10.1016/j.jcyt.2024.02.006. Epub 2024 Feb 21. Cytotherapy. 2024. PMID: 38416086
Cited by
-
Cryopreservation of Human Stem Cells for Clinical Application: A Review.Transfus Med Hemother. 2011;38(2):107-123. doi: 10.1159/000326623. Epub 2011 Mar 16. Transfus Med Hemother. 2011. PMID: 21566712 Free PMC article.
-
Systematic cryopreservation study of cardiac myoblasts in suspension.PLoS One. 2024 Mar 6;19(3):e0295131. doi: 10.1371/journal.pone.0295131. eCollection 2024. PLoS One. 2024. PMID: 38446773 Free PMC article.
-
Innovative Approach in the Cryogenic Freezing Medium for Mesenchymal Stem Cells.Biomolecules. 2022 Apr 20;12(5):610. doi: 10.3390/biom12050610. Biomolecules. 2022. PMID: 35625538 Free PMC article.
-
Comparison of the Effects of Different Cryoprotectants on Stem Cells from Umbilical Cord Blood.Stem Cells Int. 2016;2016:1396783. doi: 10.1155/2016/1396783. Epub 2015 Dec 7. Stem Cells Int. 2016. PMID: 26770201 Free PMC article.
-
Hematopoietic SCT with cryopreserved grafts: adverse reactions after transplantation and cryoprotectant removal before infusion.Bone Marrow Transplant. 2014 Apr;49(4):469-76. doi: 10.1038/bmt.2013.152. Epub 2013 Sep 30. Bone Marrow Transplant. 2014. PMID: 24076548 Free PMC article. Review.
References
-
- Wagner JE, Rosenthal J, Sweetman R, Shu XO, Davies SM, Ramsay NK, McGlave PB, Sender L, Cairo MS. Successful transplantation of HLA-matched and HLA-mismatched umbilical cord blood from unrelated donors: analysis of engraftment and acute graft-versus-host disease. Blood 1996;88:795–802. - PubMed
-
- Gluckman E, Rocha V, Boyer-Chammard A, Locatelli F, Arcese W, Pasquini R, Ortega J, Souillet G, Ferreira E, Laporte JP, Fernandez M, Chastang C. Outcome of cord-blood transplantation from related and unrelated donors. Eurocord Transplant Group and the European Blood and Marrow Transplantation Group. N Engl J Med 1997;337: 373–81. - PubMed
-
- Laughlin MJ, Barker J, Bambach B, Koc ON, Rizzieri DA, Wagner JE, Gerson SL, Lazarus HM, Cairo M, Stevens CE, Rubinstein P, Kurtzberg J. Hematopoietic engraftment and survival in adult recipients of umbilical-cord blood from unrelated donors. N Engl J Med 2001;344:1815–22. - PubMed
-
- Rubinstein P, Carrier C, Scaradavou A, Kurtzberg J, Adamson J, Migliaccio AR, Berkowitz RL, Cabbad M, Dobrila NL, Taylor PE, Rosenfield RE, Stevens CE. Outcomes among 562 recipients of placental-blood transplants from unrelated donors. N Engl J Med 1998;339:1565–77. - PubMed
-
- Barker JN, Weisdorf DJ, Wagner JE. Creation of a double chimera after the transplantation of umbilical-cord blood from two partially matched unrelated donors. N Engl J Med 2001;344:1870–1. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
