

Use of ER/PR/HER2 subtypes in conjunction with the 2007 St Gallen Consensus Statement for early breast cancer
- PMID: 20492696
- PMCID: PMC2886044
- DOI: 10.1186/1471-2407-10-228
Use of ER/PR/HER2 subtypes in conjunction with the 2007 St Gallen Consensus Statement for early breast cancer
Abstract
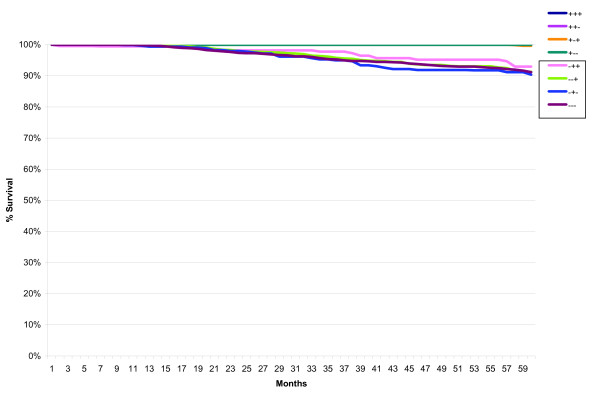
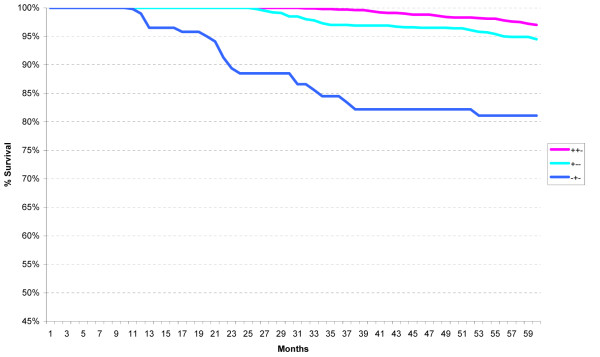
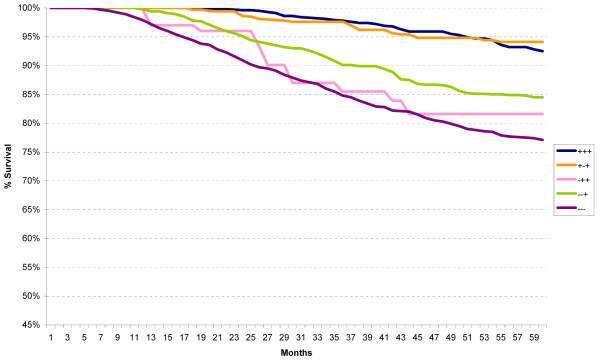
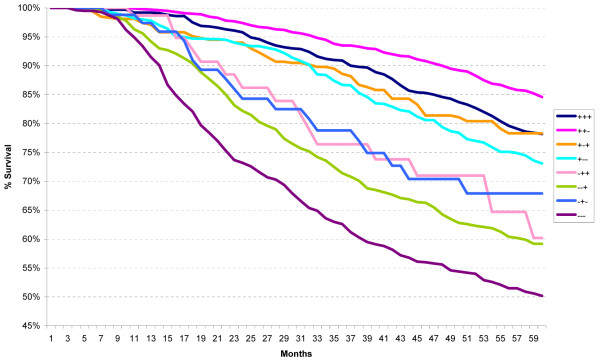
Background: The 2007 St Gallen international expert consensus statement describes three risk categories and provides recommendations for treatment of early breast cancer. The set of recommendations on how to best treat primary breast cancer is recognized and used by clinicians worldwide. We now examine the variability of five-year survival of the 2007 St Gallen Risk Classifications utilizing the ER/PR/HER2 subtypes.
Methods: Using the population-based California Cancer Registry, 114,786 incident cases of Stages 1-3 invasive breast cancer diagnosed between 2000 and 2006 were identified. Cases were assigned to Low, Intermediate, or High Risk categories. Five-year-relative survival was computed for the three St Gallen risk categories and for the ER/PR/HER2 subtypes for further differentiation.
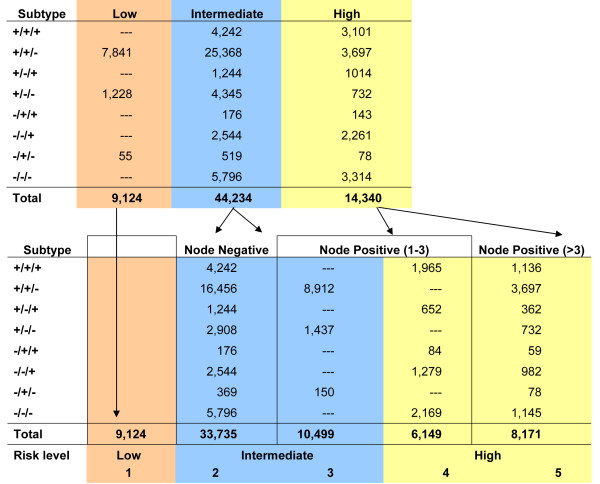
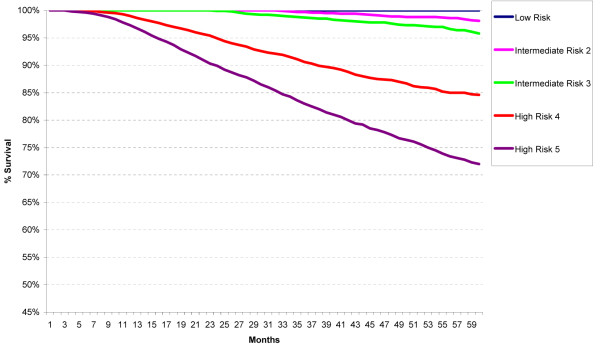
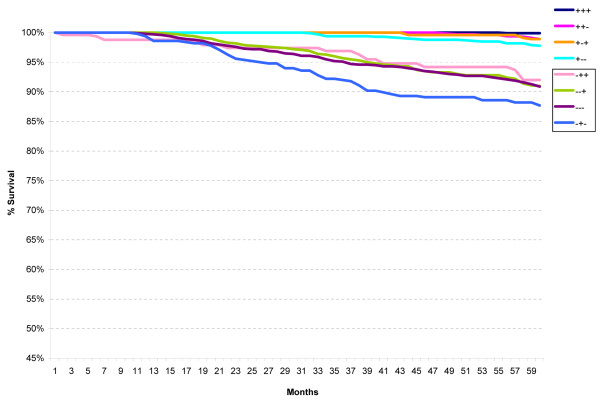
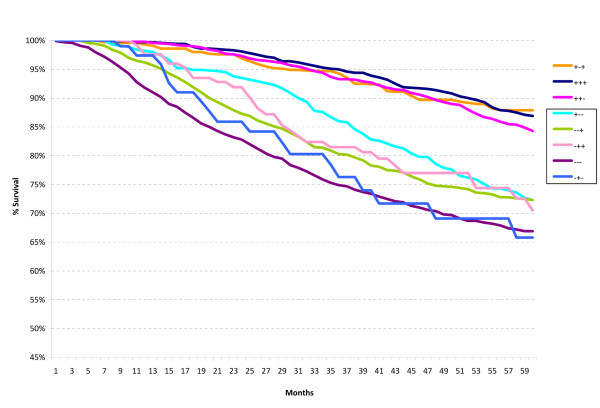
Results and discussion: There were 9,124 (13%) cases classified as Low Risk, 44,234 (65%) cases as Intermediate Risk, and 14,340 (21%) as High Risk. Within the Intermediate Risk group, 33,735 (76%) were node-negative (Intermediate Risk 2) and 10,499 (24%) were node-positive (Intermediate Risk 3). For the High Risk group, 6,149 (43%) had 1 to 3 positive axillary lymph nodes (High Risk 4) and 8,191 (57%) had four or more positive lymph nodes (High Risk 5). Using five-year relative survival as the principal criterion, we found the following: a) There was very little difference between the Low Risk and Intermediate Risk categories; b) Use of the ER/PR/HER2 subtypes within the Intermediate and High Risk categories separated each into a group with better five-year survival (ER-positive) and a group with worse survival (ER-negative), irrespective of HER2-status; c) The heterogeneity of the High Risk category was most evident when one examined the ER/PR/HER2 subtypes with four or more positive axillary lymph nodes; (d) HER2-positivity did not always translate to worse survival, as noted when one compared the triple positive subtype (ER+/PR+/HER2+) to the triple negative subtype (ER-/PR-/HER2-); and (e) ER-negativity appeared to be a stronger predictor of poor survival than HER2-positivity.
Conclusion: The use of ER/PR/HER2 subtype highlights the marked heterogeneity of the Intermediate and High Risk categories of the 2007 St Gallen statements. The use of ER/PR/HER2 subtypes and correlation with molecular classification of breast cancer is recommended.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
