

Is lymphadenectomy a prognostic marker in endometrioid adenocarcinoma of the human endometrium?
- PMID: 20492712
- PMCID: PMC2891635
- DOI: 10.1186/1471-2407-10-224
Is lymphadenectomy a prognostic marker in endometrioid adenocarcinoma of the human endometrium?
Abstract
Background: During surgery for endometrial cancer, a pelvic lymphadenectomy with or without para-aortic lymphadenectomy is performed at least in patients with risk factors (stage I, grading 2 and/or histological subtypes with higher risk of lymphatic spread), and is hence recommended by the International Federation of Obstetrics and Gynecology (FIGO). Although lymph node metastases are important prognostic parameters, it has been contentious whether a pelvic lymph node dissection itself has a prognostic impact in the treatment of endometrial cancer, especially in endometrioid adenocarcinoma. Therefore, this study evaluated whether lymphadenectomy has a prognostic impact in patients with endometrioid adenocarcinoma.
Methods: The benefits of lymphadenectomy were examined in 214 patients with a histological diagnosis of endometrial adenocarcinoma. Tumour characteristics were analysed with respect to the surgical and pathological stage.
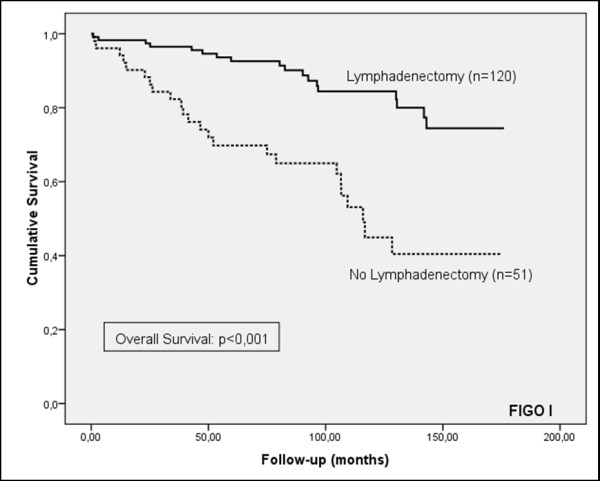
Results: Of the 214 patients with endometrial adenocarcinoma, 171 (79.9%) were classified as FIGO stage I, 15 (7.0%) FIGO stage II, 21 (9.8%) FIGO stage III and 7 (3.3%) FIGO stage IV. One hundred and thirty four (62.6%) of the patients had a histological grade 1 tumour, while 56 (26.2%) and 24 (11.2%) had a histological grade 2 or grade 3 tumour, respectively. Lymphadenectomy was performed in 151 (70.6%) patients. Only 11 (5.1%) patients showed metastatic disease in the lymph nodes. The performance of a lymphadenectomy resulted in significantly increased cause-specific and overall survival, while progression-free survival was not affected by this operative procedure.
Conclusions: The performance of an operative lymphadenectomy resulted in better survival of patients with endometrioid adenocarcinoma. This increase was significant for cause-specific and overall survival, while there was a tendency only towards increased progression-free survival. Therefore, even in endometrioid adenocarcinoma, a pelvic and/or para-aortic lymphadenectomy should be performed.
Figures





Similar articles
-
Lymphadenectomy and prognosis for elderly females with stage I endometrioid endometrial cancer.Arch Gynecol Obstet. 2019 Sep;300(3):683-691. doi: 10.1007/s00404-019-05225-6. Epub 2019 Jun 29. Arch Gynecol Obstet. 2019. PMID: 31256231
-
Survival impact based on the thoroughness of pelvic lymphadenectomy in intermediate- or high-risk groups of endometrioid-type endometrial cancer: A multi-center retrospective cohort analysis.Gynecol Oncol. 2016 Jun;141(3):440-446. doi: 10.1016/j.ygyno.2016.03.031. Epub 2016 Apr 8. Gynecol Oncol. 2016. PMID: 27020700
-
The prognostic significance of aortic lymph node metastasis in endometrial cancer: Potential implications for selective aortic lymph node assessment.Gynecol Oncol. 2019 Jun;153(3):505-510. doi: 10.1016/j.ygyno.2019.03.251. Epub 2019 Mar 30. Gynecol Oncol. 2019. PMID: 30935714 Free PMC article.
-
Staging for endometrial cancer: The controversy around lymphadenectomy - Can this be resolved?Best Pract Res Clin Obstet Gynaecol. 2015 Aug;29(6):845-57. doi: 10.1016/j.bpobgyn.2015.02.007. Epub 2015 Mar 4. Best Pract Res Clin Obstet Gynaecol. 2015. PMID: 25817745 Review.
-
Combined pelvic and para-aortic is superior to only pelvic lymphadenectomy in intermediate and high-risk endometrial cancer: a systematic review and meta-analysis.Arch Gynecol Obstet. 2020 Jul;302(1):249-263. doi: 10.1007/s00404-020-05587-2. Epub 2020 May 28. Arch Gynecol Obstet. 2020. PMID: 32468162
Cited by
-
Major regulators of microRNAs biogenesis Dicer and Drosha are down-regulated in endometrial cancer.Tumour Biol. 2011 Aug;32(4):769-76. doi: 10.1007/s13277-011-0179-0. Epub 2011 May 11. Tumour Biol. 2011. PMID: 21559780 Free PMC article.
-
Therapeutic role of systematic lymphadenectomy in early-stage endometrial cancer: A systematic review.Oncol Lett. 2016 Jun;11(6):3849-3857. doi: 10.3892/ol.2016.4467. Epub 2016 Apr 19. Oncol Lett. 2016. PMID: 27313706 Free PMC article.
-
Survival advantage of lymphadenectomy in endometrial cancer.J Cancer Res Clin Oncol. 2016 May;142(5):1051-60. doi: 10.1007/s00432-015-2109-9. Epub 2016 Jan 8. J Cancer Res Clin Oncol. 2016. PMID: 26746654 Free PMC article.
References
-
- FIGO stages (announcements) Gynecol Oncol. 1989;35:125–127. doi: 10.1016/0090-8258(89)90027-9. - DOI
-
- Morrow CP, Bundy BN, Kurman RJ, Creasman WT, Heller P, Homesley HD, Graham JE. Relationship between surgical-pathological risk factors and outcome in clinical stage I and II carcinoma of the endometrium: a Gynecologic Oncology Group study. Gynecol Oncol. 1991;40(1):55–65. doi: 10.1016/0090-8258(91)90086-K. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
