

Haploinsufficiency of TAB2 causes congenital heart defects in humans
- PMID: 20493459
- PMCID: PMC3032066
- DOI: 10.1016/j.ajhg.2010.04.011
Haploinsufficiency of TAB2 causes congenital heart defects in humans
Abstract
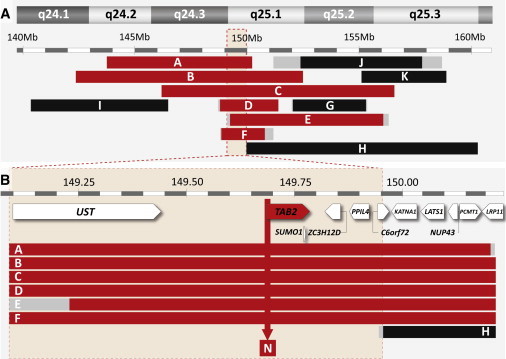
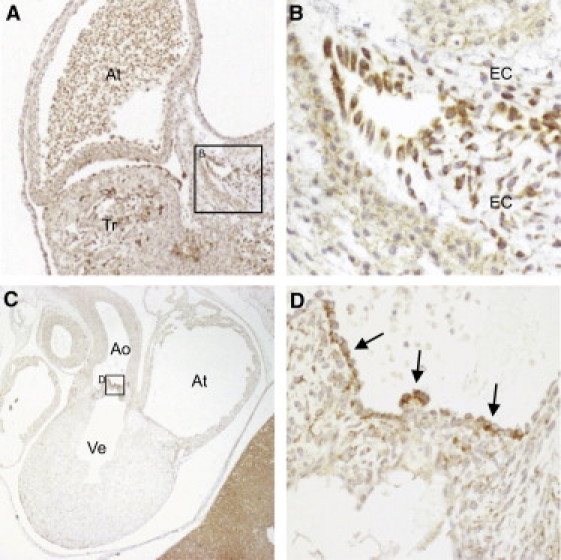
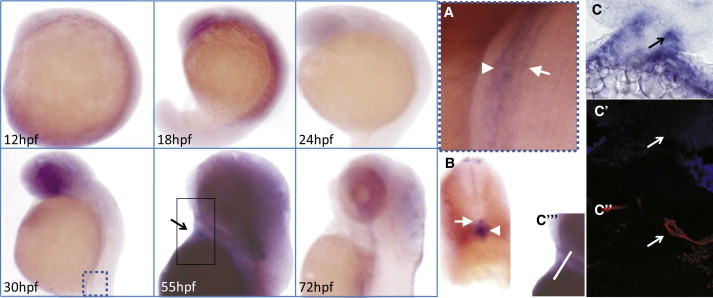
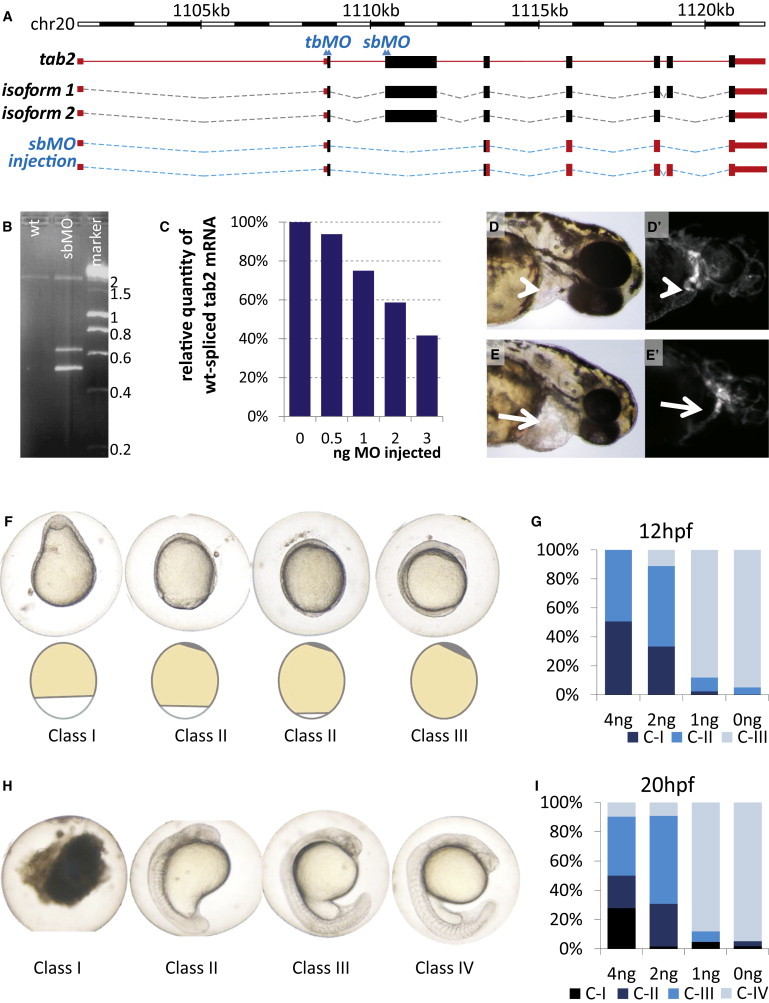
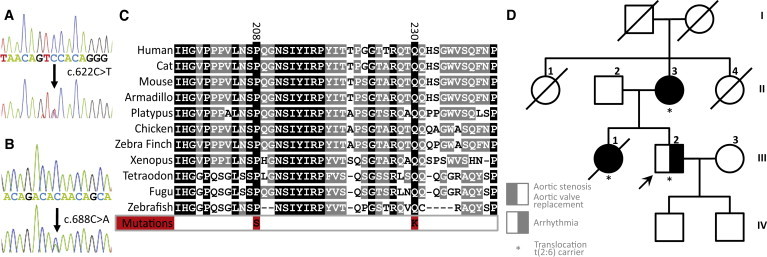
Congenital heart defects (CHDs) are the most common major developmental anomalies and the most frequent cause for perinatal mortality, but their etiology remains often obscure. We identified a locus for CHDs on 6q24-q25. Genotype-phenotype correlations in 12 patients carrying a chromosomal deletion on 6q delineated a critical 850 kb region on 6q25.1 harboring five genes. Bioinformatics prioritization of candidate genes in this locus for a role in CHDs identified the TGF-beta-activated kinase 1/MAP3K7 binding protein 2 gene (TAB2) as the top-ranking candidate gene. A role for this candidate gene in cardiac development was further supported by its conserved expression in the developing human and zebrafish heart. Moreover, a critical, dosage-sensitive role during development was demonstrated by the cardiac defects observed upon titrated knockdown of tab2 expression in zebrafish embryos. To definitively confirm the role of this candidate gene in CHDs, we performed mutation analysis of TAB2 in 402 patients with a CHD, which revealed two evolutionarily conserved missense mutations. Finally, a balanced translocation was identified, cosegregating with familial CHD. Mapping of the breakpoints demonstrated that this translocation disrupts TAB2. Taken together, these data clearly demonstrate a role for TAB2 in human cardiac development.
Copyright 2010 The American Society of Human Genetics. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Familial TAB2 microdeletion and congenital heart defects including unusual valve dysplasia and tetralogy of fallot.Am J Med Genet A. 2015 Nov;167A(11):2702-6. doi: 10.1002/ajmg.a.37210. Epub 2015 Jul 2. Am J Med Genet A. 2015. PMID: 26139517
-
A novel TAB2 nonsense mutation (p.S149X) causing autosomal dominant congenital heart defects: a case report of a Chinese family.BMC Cardiovasc Disord. 2020 Jan 20;20(1):27. doi: 10.1186/s12872-019-01322-1. BMC Cardiovasc Disord. 2020. PMID: 31959127 Free PMC article.
-
6q25.1 (TAB2) microdeletion is a risk factor for hypoplastic left heart: a case report that expands the phenotype.BMC Cardiovasc Disord. 2020 Mar 17;20(1):137. doi: 10.1186/s12872-020-01404-5. BMC Cardiovasc Disord. 2020. PMID: 32183715 Free PMC article.
-
Using Zebrafish to Analyze the Genetic and Environmental Etiologies of Congenital Heart Defects.Adv Exp Med Biol. 2020;1236:189-223. doi: 10.1007/978-981-15-2389-2_8. Adv Exp Med Biol. 2020. PMID: 32304074 Review.
-
Zebrafish Congenital Heart Disease Models: Opportunities and Challenges.Int J Mol Sci. 2024 May 29;25(11):5943. doi: 10.3390/ijms25115943. Int J Mol Sci. 2024. PMID: 38892128 Free PMC article. Review.
Cited by
-
A hypomorphic lsd1 allele results in heart development defects in mice.PLoS One. 2013 Apr 24;8(4):e60913. doi: 10.1371/journal.pone.0060913. Print 2013. PLoS One. 2013. PMID: 23637775 Free PMC article.
-
Computational tools for prioritizing candidate genes: boosting disease gene discovery.Nat Rev Genet. 2012 Jul 3;13(8):523-36. doi: 10.1038/nrg3253. Nat Rev Genet. 2012. PMID: 22751426 Review.
-
Prioritization of candidate genes for attention deficit hyperactivity disorder by computational analysis of multiple data sources.Protein Cell. 2012 Jul;3(7):526-34. doi: 10.1007/s13238-012-2931-7. Epub 2012 Jul 10. Protein Cell. 2012. PMID: 22773342 Free PMC article.
-
A Comprehensive Genomic Analysis Reveals the Genetic Landscape of Mitochondrial Respiratory Chain Complex Deficiencies.PLoS Genet. 2016 Jan 7;12(1):e1005679. doi: 10.1371/journal.pgen.1005679. eCollection 2016 Jan. PLoS Genet. 2016. PMID: 26741492 Free PMC article.
-
Genetic Etiology of Left-Sided Obstructive Heart Lesions: A Story in Development.J Am Heart Assoc. 2021 Jan 19;10(2):e019006. doi: 10.1161/JAHA.120.019006. Epub 2021 Jan 12. J Am Heart Assoc. 2021. PMID: 33432820 Free PMC article. Review.
References
-
- Hoffman J.I., Kaplan S. The incidence of congenital heart disease. J. Am. Coll. Cardiol. 2002;39:1890–1900. - PubMed
-
- Thom T., Haase N., Rosamond W., Howard V.J., Rumsfeld J., Manolio T., Zheng Z.J., Flegal K., O'Donnell C., Kittner S., American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113:e85–e151. - PubMed
-
- Jenkins K.J., Correa A., Feinstein J.A., Botto L., Britt A.E., Daniels S.R., Elixson M., Warnes C.A., Webb C.L., American Heart Association Council on Cardiovascular Disease in the Young Noninherited risk factors and congenital cardiovascular defects: current knowledge: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young: endorsed by the American Academy of Pediatrics. Circulation. 2007;115:2995–3014. - PubMed
-
- Calcagni G., Digilio M.C., Sarkozy A., Dallapiccola B., Marino B. Familial recurrence of congenital heart disease: an overview and review of the literature. Eur. J. Pediatr. 2007;166:111–116. - PubMed
-
- Manning N., Archer N. A study to determine the incidence of structural congenital heart disease in monochorionic twins. Prenat. Diagn. 2006;26:1062–1064. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
