

Review
doi: 10.1016/j.jcrs.2010.03.025.
Femtosecond laser in laser in situ keratomileusis
Affiliations
- PMID: 20494777
- PMCID: PMC4089871
- DOI: 10.1016/j.jcrs.2010.03.025
Item in Clipboard
Review
Femtosecond laser in laser in situ keratomileusis
J Cataract Refract Surg.
2010 Jun.
Abstract
Flap creation is a critical step in laser in situ keratomileusis (LASIK). Efforts to improve the safety and predictability of the lamellar incision have fostered the development of femtosecond lasers. Several advantages of the femtosecond laser over mechanical microkeratomes have been reported in LASIK surgery. In this article, we review common considerations in management and complications of this step in femtosecond laser-LASIK and concentrate primarily on the IntraLase laser because most published studies relate to this instrument.
(c) 2010 ASCRS and ESCRS. Published by Elsevier Inc. All rights reserved.
Figures
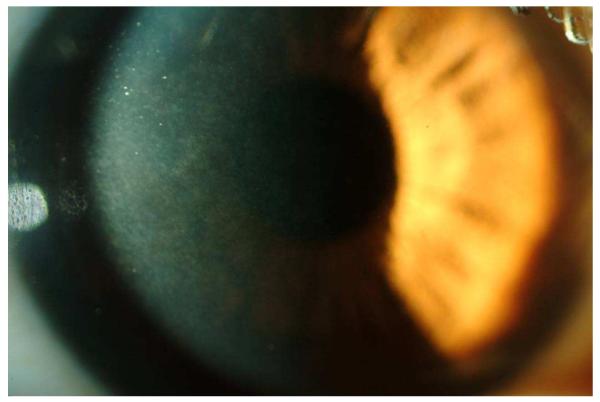
Slitlamp photograph showing trace interface haze after ultrathin-flap (90 μm) femtosecond laser LASIK. Although the patient had no decrease in CDVA, a light-scattering test (C-Quant) was abnormal in the eye (courtesy of Karolinne M. Rocha, MD).
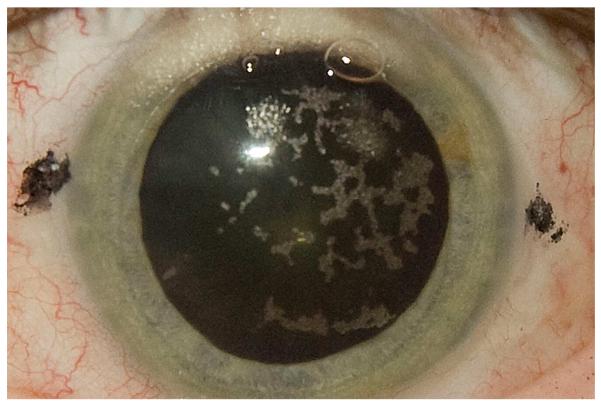
Diffuse OBL 5 minutes after flap creation using the IntraLase 60 kHz femtosecond laser. Over 35 minutes, all the bubbles were cleared from the cornea and refractive ablation was performed with no interference with the tracking system of the excimer laser.
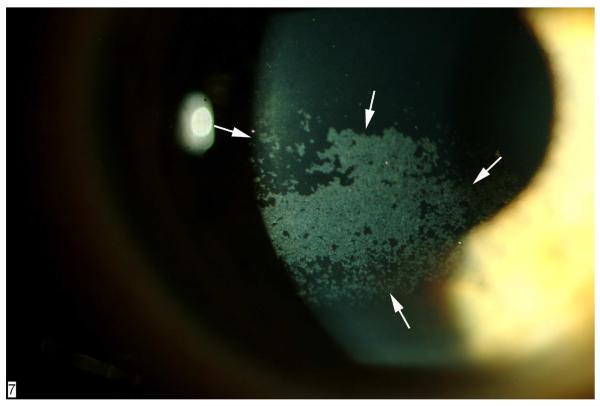
Slitlamp documentation of severe punctate epithelial erosions (arrows) in the cornea of an eye that developed LASIK-induced neurotrophic epitheliopathy 1 week after surgery. The epitheliopathy involved the pupillary area, and there was some decrease in CDVA, which resolved 6 months after surgery.
References
-
- Barraquer JI. Basis of refractive keratoplasty—1967. Refract Corneal Surg. 1989;5:179–193. - PubMed
-
- Pallikaris IG, Papatzanaki ME, Stathi EZ, Frenschock O, Georgiadis A. Laser in situ keratomileusis. Lasers Surg Med. 1990;10:463–468. - PubMed
-
- Pallikaris IG, Papatzanaki ME, Siganos DS, Tsilimbaris MK. A corneal flap technique for laser in situ keratomileusis; human studies. Arch Ophthalmol. 1991;109:1699–1702. - PubMed
-
- Buratto L, Ferrari M, Rama P. Excimer laser intrastromal keratomileusis. Am J Ophthalmol. 1992;113:291–295. - PubMed
-
- Ambrósio R, Jr, Wilson SE. LASIK vs LASEK vs PRK: advantages and indications. Semin Ophthalmol. 2003;18:2–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
