

Potent anti-ischaemic effects of statins in chronic stable angina: incremental benefit beyond lipid lowering?
- PMID: 20494902
- PMCID: PMC2966969
- DOI: 10.1093/eurheartj/ehq133
Potent anti-ischaemic effects of statins in chronic stable angina: incremental benefit beyond lipid lowering?
Abstract
Aims: The DoUble-blind Atorvastatin AmLodipine (DUAAL) trial investigated whether atorvastatin decreases ischaemia by a vascular benefit, independent of low-density lipoprotein cholesterol lowering, in patients with coronary artery disease (CAD), both alone and in combination with the traditional anti-anginal therapy, amlodipine.
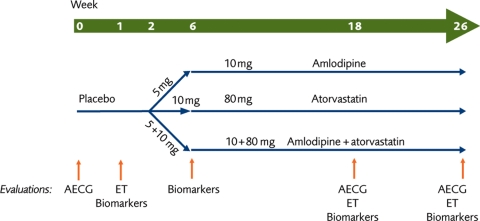
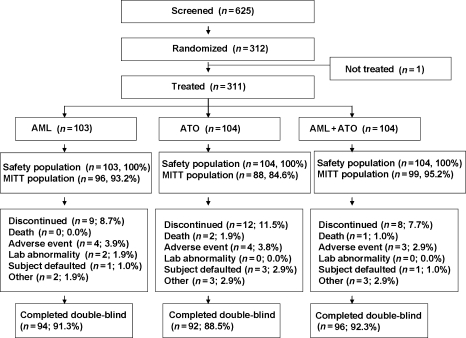
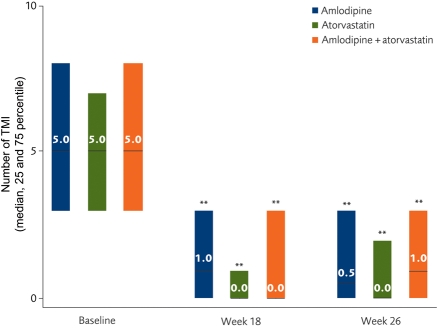
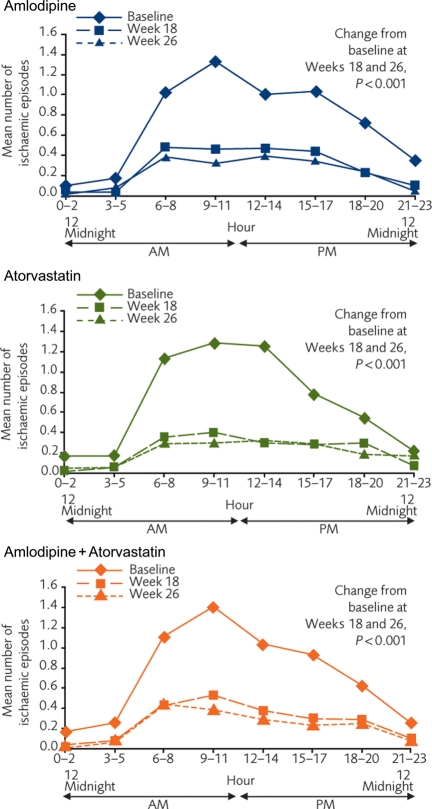
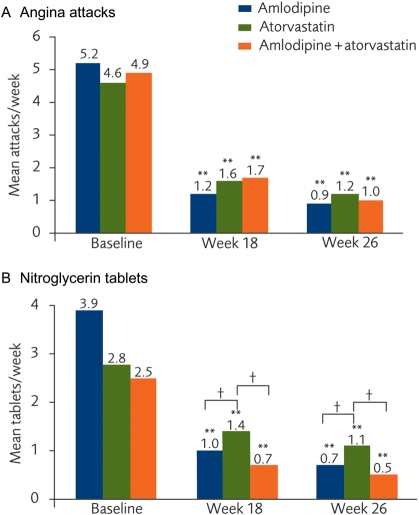
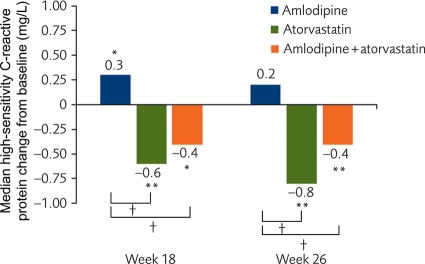
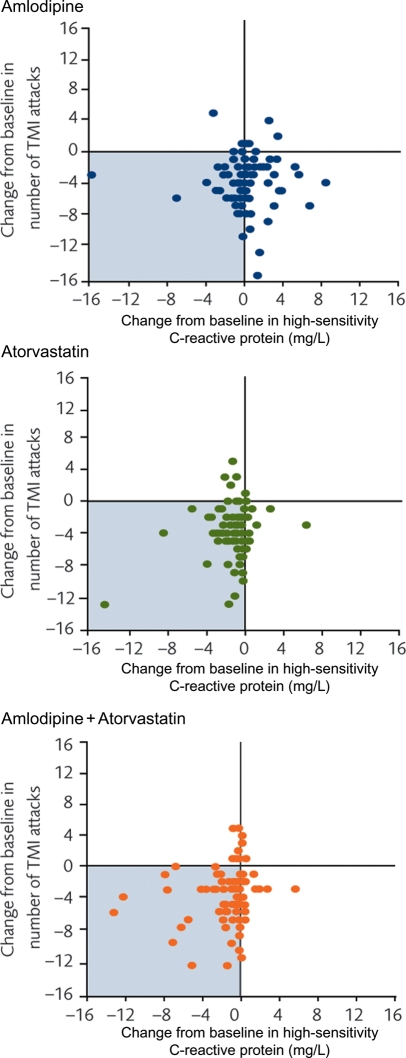
Methods and results: Randomized, double-blind, parallel-group, multicountry trial (2 weeks run-in and 24 weeks active therapy) comparing three treatments: amlodipine, atorvastatin, and amlodipine + atorvastatin; in 311 patients (78% male; mean age 62 years) with stable angina (≥ 2 attacks/week), CAD history, ≥ 3 transient myocardial ischaemia (TMI) episodes, and/or ≥ 15 min ischaemia on 48 h ambulatory electrocardiographic (AECG) monitoring. Efficacy variables were change in TMI by AECG, exercise ischaemia, angina diary data, and inflammatory biomarkers at Week 26. There was a comparable, highly significant decrease in TMI with amlodipine and atorvastatin, but no additional benefit for the combination. More than 50% of patients became TMI-free in all three groups and this was accompanied by a comparable, marked reduction in angina and nitroglycerin consumption. High-sensitivity C-reactive protein fell by 40% in patients receiving atorvastatin but there was no change with amlodipine. Adverse events were comparable among groups.
Conclusion: Atorvastatin was as potent an anti-ischaemic agent as amlodipine. Future studies of combination therapies will be instructive.
Clinical trial registration information: National clinical trial number: NCT00159718, protocol number A0531031 listed on http://clinicaltrials.gov/.
Figures
Comment in
-
Has atorvastatin more than a DUAAL face?Eur Heart J. 2010 Nov;31(21):2567-8. doi: 10.1093/eurheartj/ehq214. Epub 2010 Jul 8. Eur Heart J. 2010. PMID: 20616096 No abstract available.
References
-
- Shaw LJ, Berman DS, Maron DJ, Mancini GB, Hayes SW, Hartigan PM, Weintraub WS, O'Rourke RA, Dada M, Spertus JA, Chaitman BR, Friedman J, Slomka P, Heller GV, Germano G, Gosselin G, Berger P, Kostuk WJ, Schwartz RG, Knudtson M, Veledar E, Bates ER, McCallister B, Teo KK, Boden WE. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117:1283–1291. doi:10.1161/CIRCULATIONAHA.107.743963. - DOI - PubMed
-
- Libby P. Inflammation and cardiovascular disease mechanisms. Am J Clin Nutr. 2006;83:456S–460S. - PubMed
-
- Deedwania PC, Carbajal EV. Silent ischemia during daily life is an independent predictor of mortality in stable angina. Circulation. 1990;81:748–756. - PubMed
-
- Deanfield JE, Detry JM, Lichtlen PR, Magnani B, Sellier P, Thaulow E. Amlodipine reduces transient myocardial ischemia in patients with coronary artery disease: double-blind Circadian Anti-Ischemia Program in Europe (CAPE Trial) J Am Coll Cardiol. 1994;24:1460–1467. - PubMed
-
- Deedwania PC, Carbajal EV. Prevalence and patterns of silent myocardial ischemia during daily life in stable angina patients receiving conventional antianginal drug therapy. Am J Cardiol. 1990;65:1090–1096. doi:10.1016/0002-9149(90)90319-V. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
