

Systematic review of randomized controlled trials of pharmacological interventions to reduce ischaemia-reperfusion injury in elective liver resection with vascular occlusion
- PMID: 20495639
- PMCID: PMC2814398
- DOI: 10.1111/j.1477-2574.2009.00120.x
Systematic review of randomized controlled trials of pharmacological interventions to reduce ischaemia-reperfusion injury in elective liver resection with vascular occlusion
Abstract
Background: Vascular occlusion during liver resection results in ischaemia-reperfusion (IR) injury, which can lead to liver dysfunction. We performed a systematic review and meta-analysis to assess the benefits and harms of using various pharmacological agents to decrease IR injury during liver resection with vascular occlusion.
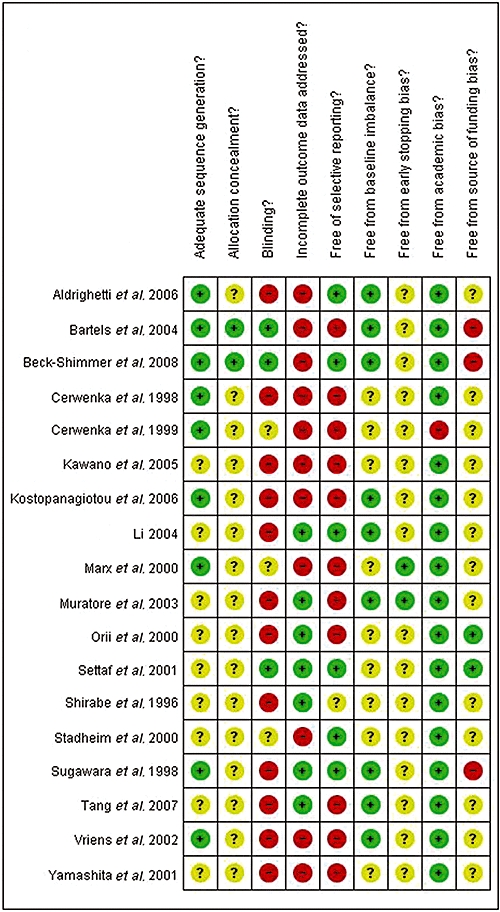
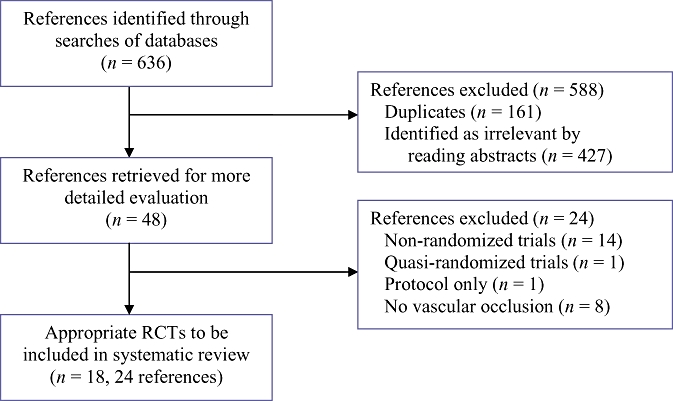
Methods: Randomized clinical trials (RCTs) evaluating pharmacological agents in liver resections conducted under vascular occlusion were identified. Two independent reviewers extracted data on population characteristics and risk of bias in the trials, and on outcomes such as postoperative morbidity, hospital stay and liver function.
Results: A total of 18 RCTs evaluating 17 different pharmacological interventions were identified. There was no significant difference in perioperative mortality, liver failure or postoperative morbidity between the intervention and control groups in any of the comparisons. A significant improvement in liver function was seen with methylprednisolone use. Hospital and intensive therapy unit stay were significantly shortened with trimetazidine and vitamin E use, respectively. Markers of liver parenchymal injury were significantly lower in the methylprednisolone, trimetazidine, dextrose and ulinastatin groups compared with their respective controls (placebo or no intervention).
Discussion: Methylprednisolone, trimetazidine, dextrose and ulinastatin may have protective roles against IR injury in liver resection. However, based on the current evidence, they cannot be recommended for routine use and their application should be restricted to RCTs.
Figures
References
-
- Chouker A, Martignoni A, Schauer R, Dugas M, Rau HG, Jauch KW, et al. Beneficial effects of ischaemic preconditioning in patients undergoing hepatectomy: the role of neutrophils. Arch Surg. 2005;140:129–136. - PubMed
-
- Hospital Episode Statistics. Main operations. 3 character: 2004–05. http://www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937&categ.... [Accessed 17 April 2007.
-
- Ibrahim S, Chen CL, Lin CC, Yang CH, Wang CC, Wang SH, et al. Intraoperative blood loss is a risk factor for complications in donors after living donor hepatectomy. Liver Transplant. 2006;12:950–957. - PubMed
-
- Shimada M, Takenaka K, Fujiwara Y, Gion T, Shirabe K, Yanaga K, et al. Risk factors linked to postoperative morbidity in patients with hepatocellular carcinoma. Br J Surg. 1998;85:195–198. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
