

Alpha-fetoprotein and tumour size are associated with microvascular invasion in explanted livers of patients undergoing transplantation with hepatocellular carcinoma
- PMID: 20495646
- PMCID: PMC2814405
- DOI: 10.1111/j.1477-2574.2009.00128.x
Alpha-fetoprotein and tumour size are associated with microvascular invasion in explanted livers of patients undergoing transplantation with hepatocellular carcinoma
Abstract
Background: To determine factors associated with outcomes and microvascular invasion (MVI) in patients undergoing liver transplantation (LT) for hepatocellular carcinoma (HCC).
Methods: Between July 1996 and August 2008 at the Universities of Kentucky or Tennessee, LT recipients were retrospectively analysed.
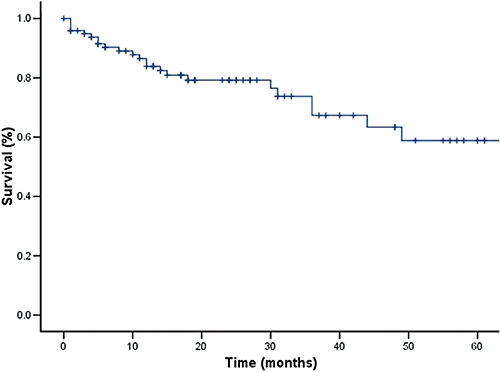
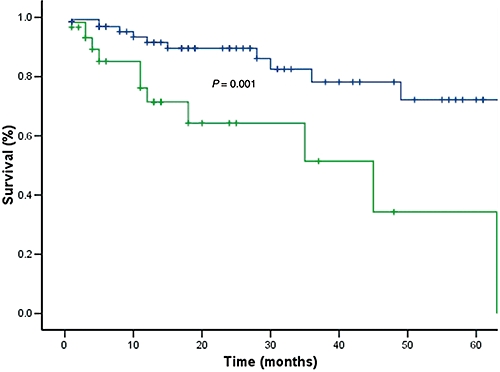
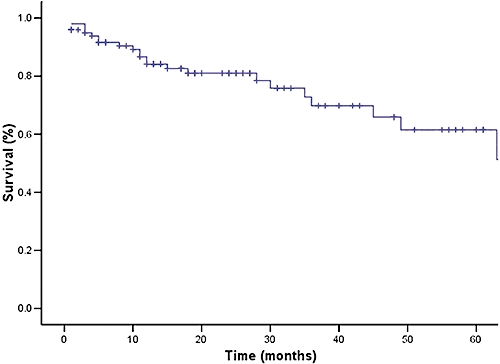
Results: One hundred and one patients had HCC in the explanted liver; one patient was excluded because of fibrolamellar histology. Seventy-nine (79%) were male and 81 (81%) were older than 50. HCC was incidental in 32 patients (32%). Median follow-up was 31 months. Ten patients (10%) developed recurrence, which was associated with poor survival (P= 0.006). Overall 1-, 3-, and 5-year survival rates were 87%, 69% and 62%, respectively. Excluding patients with lymph node metastasis (LNM) or MVI yielded 91%, 81% and 75% survival at the same time points. MVI was independently associated with recurrence (OR 28.40, 95% CI 1.77-456.48, P= 0.018) and decreased survival (OR 4.70, 95% CI 1.24-17.80, P= 0.023), and LNM with decreased survival (OR 6.05, 95% CI 1.23-29.71, P= 0.027). Tumour size (OR 4.1, 95% CI 1.2-13.5, P= 0.013) and alpha-fetoprotein (AFP) > 100 (OR 5.0, 95% CI 1.4-18.1, P= 0.006) were associated with MVI.
Conclusions: MVI greatly increases the risk of recurrence and death after LT for HCC, and is strongly associated with tumour size and AFP > 100.
Figures
References
-
- Caldwell S, Park SH. The epidemiology of hepatocellular cancer: from the perspectives of public health problem to tumor biology. J Gastroenterol. 2009;44(Suppl. 19):96–101. - PubMed
-
- Penn I. Hepatic transplantation for primary and metastatic cancers of the liver. Surgery. 1991;110:726–734. discussion 34-5. - PubMed
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
