

Neoadjuvant therapy may lead to successful surgical resection and improved survival in patients with borderline resectable pancreatic cancer
- PMID: 20495649
- PMCID: PMC2814408
- DOI: 10.1111/j.1477-2574.2009.00136.x
Neoadjuvant therapy may lead to successful surgical resection and improved survival in patients with borderline resectable pancreatic cancer
Abstract
Background: Borderline resectable pancreatic cancers are technically amenable to surgical resection, but are associated with increased risk of locoregional recurrence. Patients with these tumours may be treated with neoadjuvant therapy in an attempt to improve margin-negative resection rates.
Methods: The University of Cincinnati Pancreatic Cancer Database was retrospectively reviewed. Borderline resectable disease was defined by the following radiographic criteria: (i) short segment occlusion of the superior mesenteric vein (SMV), portal vein (PV) or SMV/PV confluence; (ii) short segment hepatic artery encasement, or (iii) superior mesenteric artery/coeliac artery abutment of <180 degrees. Patients with resectable disease who had questionable metastatic disease or poor performance status were also included.
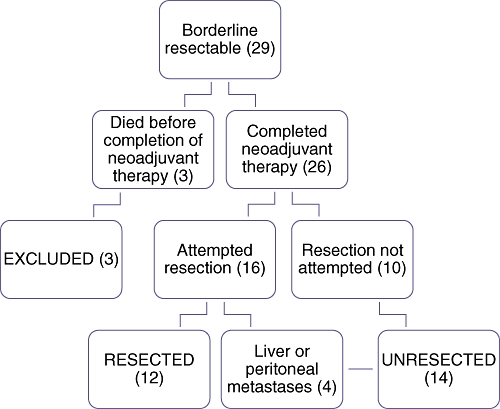
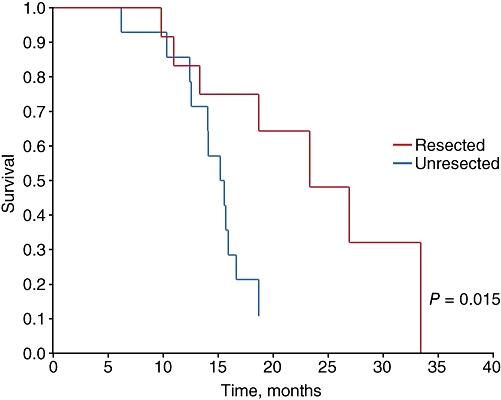
Results: Twenty-nine patients met the criteria. Of these, 26 underwent a full course of neoadjuvant therapy. Twelve (46%) underwent surgical resection and 14 had tumour progression or were deemed unresectable at laparotomy. The most common neoadjuvant therapy regimen was gemcitabine-based chemotherapy alone (58%). Of those undergoing surgery, 67% had margin-negative (R0) resections and 42% required venous resection. Median survival was 15.5 months for unresected patients and 23.3 months for resected patients.
Discussion: Borderline resectable pancreatic tumours can be treated neoadjuvantly, resulting in margin-negative resection and survival rates similar to those in initially resectable disease.
Figures
References
-
- Varadhachary GR, Tamm EP, Abbruzzese JL, Xiong HQ, Crane CH, Wang H, et al. Borderline resectable pancreatic cancer: definitions, management, and role of preoperative therapy. Ann Surg Oncol. 2006;13:1035–1046. - PubMed
-
- National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Pancreatic Adenocarcinoma. v.1.2008. http://www.nccn.org/professionals/physician_gls/default.asp. [Accessed 1 February 2009]
-
- Ahmad SA, Lowy AM, McIntyre BC, Matthews JB. Pancreaticoduodenectomy. J Gastrointest Surg. 2005;9:138–143. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
