

A diagnostic paradigm for resectable liver lesions: to biopsy or not to biopsy?
- PMID: 20495704
- PMCID: PMC2785947
- DOI: 10.1111/j.1477-2574.2009.00081.x
A diagnostic paradigm for resectable liver lesions: to biopsy or not to biopsy?
Abstract
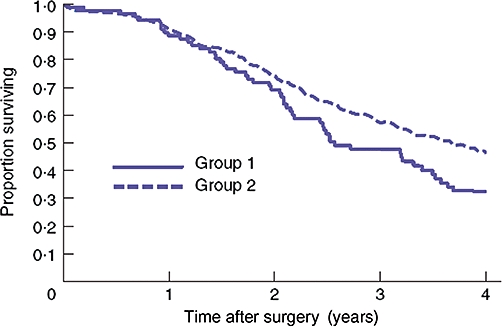
Background: Despite a growing body of evidence reporting the deleterious mechanical and oncological complications of biopsy of hepatic malignancy, a small but significant number of patients undergo the procedure prior to specialist surgical referral. Biopsy has been shown to result in poorer longterm survival following resection and advances in modern imaging modalities provide equivalent, or better, diagnostic accuracy.
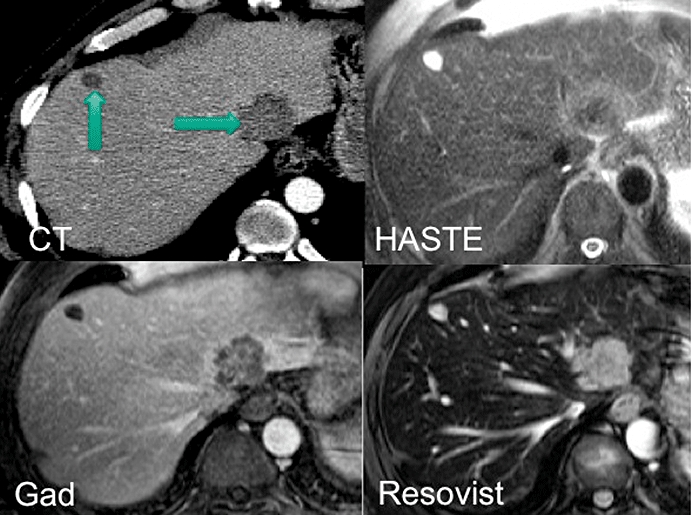
Methods: The literature relating to needle-tract seeding of primary and secondary liver cancers was reviewed. MEDLINE, EMBASE and the Cochrane Library were searched for case reports and series relating to the oncological complications of biopsy of liver malignancies. Current non-invasive diagnostic modalities are reviewed and their diagnostic accuracy presented.
Results: Biopsy of malignant liver lesions has been shown to result in poorer longterm survival following resection and does not confer any diagnostic advantage over a combination of non-invasive imaging techniques and serum tumour markers.
Conclusions: Given that chemotherapeutic advances now often permit downstaging and subsequent resection of 'unresectable' disease, the time has come to abandon biopsy of solid lesions outside the setting of a specialist multi-disciplinary team meeting (MDT).
Figures
Similar articles
-
Pretherapeutic evaluation of patients with upper gastrointestinal tract cancer using endoscopic and laparoscopic ultrasonography.Dan Med J. 2012 Dec;59(12):B4568. Dan Med J. 2012. PMID: 23290296 Review.
-
Comparison of a coaxial versus non-coaxial liver biopsy technique in an oncological setting: diagnostic yield, complications and seeding risk.Eur Radiol. 2020 Dec;30(12):6702-6708. doi: 10.1007/s00330-020-07038-7. Epub 2020 Jul 14. Eur Radiol. 2020. PMID: 32666317 Free PMC article.
-
Is Core Needle Biopsy Reliable in Differentiating Between Aggressive Benign and Malignant Radiolucent Bone Tumors?Clin Orthop Relat Res. 2018 Mar;476(3):568-577. doi: 10.1007/s11999.0000000000000062. Clin Orthop Relat Res. 2018. PMID: 29529643 Free PMC article.
-
Management of undifferentiated embryonal sarcoma of the liver in children: a case series and management review.S Afr Med J. 2013 Jun 27;103(10):728-31. doi: 10.7196/samj.6058. S Afr Med J. 2013. PMID: 24079623
-
Tissue diagnosis of suspected lung cancer: selecting between bronchoscopy, transthoracic needle aspiration, and resectional biopsy.Respir Care Clin N Am. 2003 Mar;9(1):51-76. doi: 10.1016/s1078-5337(02)00083-7. Respir Care Clin N Am. 2003. PMID: 12820712 Review.
Cited by
-
Solitary fibrous tumour of the liver-report on metastasis and local recurrence of a malignant case and review of literature.World J Surg Oncol. 2017 Jan 18;15(1):27. doi: 10.1186/s12957-017-1102-y. World J Surg Oncol. 2017. PMID: 28100235 Free PMC article. Review.
-
Biopsy and puncture track metastasis.Dtsch Arztebl Int. 2013 Jan;110(4):59. doi: 10.3238/arztebl.2013.0059b. Epub 2013 Jan 25. Dtsch Arztebl Int. 2013. PMID: 23413392 Free PMC article. No abstract available.
-
Contrast-enhanced ultrasound (CEUS): one step forward in the identification of "high risk" solitary fibrotic tumors of the liver.J Ultrasound. 2024 Dec;27(4):921-925. doi: 10.1007/s40477-024-00890-z. Epub 2024 Apr 10. J Ultrasound. 2024. PMID: 38598134
-
Changing role of histopathology in the diagnosis and management of hepatocellular carcinoma.World J Gastroenterol. 2018 Sep 21;24(35):4000-4013. doi: 10.3748/wjg.v24.i35.4000. World J Gastroenterol. 2018. PMID: 30254404 Free PMC article. Review.
-
Operative terminology and post-operative management approaches applied to hepatic surgery: Trainee perspectives.World J Gastrointest Surg. 2013 May 27;5(5):146-55. doi: 10.4240/wjgs.v5.i5.146. World J Gastrointest Surg. 2013. PMID: 23710292 Free PMC article.
References
-
- Chun YS, Vauthey JN. Extending the frontiers of resectability in advanced colorectal cancer. Eur J Surg Oncol. 2007;33(Suppl. 2):52–58. - PubMed
-
- Jones OM, Rees M, John TG, Bygrave S, Plant G. Biopsy of resectable colorectal liver metastases causes tumour dissemination and adversely affects survival after liver resection. Br J Surg. 2005;92:1165–1168. - PubMed
-
- Ryd W, Hagmar B, Eriksson O. Local tumour cell seeding by fine-needle aspiration biopsy. A semi-quantitative study. Acta Pathol Microbiol Immunol Scand [A] 1983;91:17–21. - PubMed
LinkOut - more resources
Full Text Sources
