

Quantification of left ventricular remodeling in response to isolated aortic or mitral regurgitation
- PMID: 20497540
- PMCID: PMC2893171
- DOI: 10.1186/1532-429X-12-32
Quantification of left ventricular remodeling in response to isolated aortic or mitral regurgitation
Abstract
Background: The treatment of patients with aortic regurgitation (AR) or mitral regurgitation (MR) relies on the accurate assessment of the severity of the regurgitation as well as its effect on left ventricular (LV) size and function. Cardiovascular Magnetic Resonance (CMR) is an excellent tool for quantifying regurgitant volumes as well as LV size and function. The 2008 AHA/ACC management guidelines for the therapy of patients with AR or MR only describe LV size in terms of linear dimensions (i.e. end-diastolic and end-systolic dimension). LV volumes that correspond to these linear dimensions have not been published in the peer-reviewed literature. The purpose of this study is to determine the effect of regurgitant volume on LV volumes and chamber dimensions in patients with isolated AR or MR and preserved LV function.
Methods: Regurgitant volume, LV volume, mass, linear dimensions, and ejection fraction, were determined in 34 consecutive patients with isolated AR and 23 consecutive patients with MR and no other known cardiac disease.
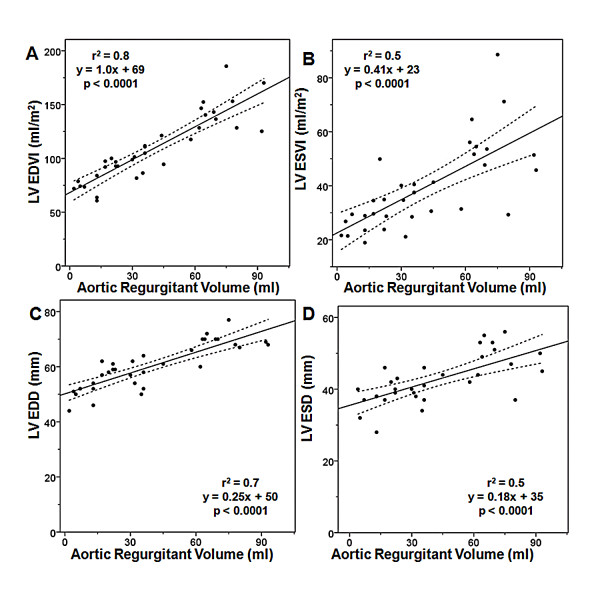
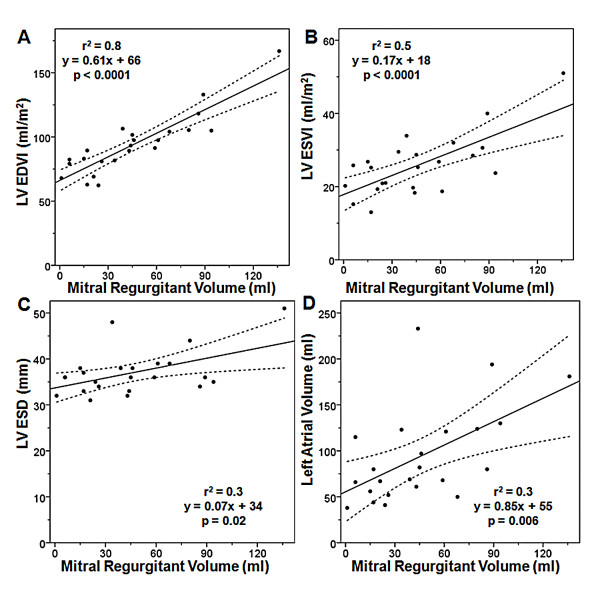
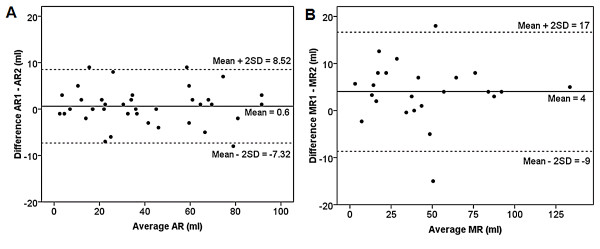
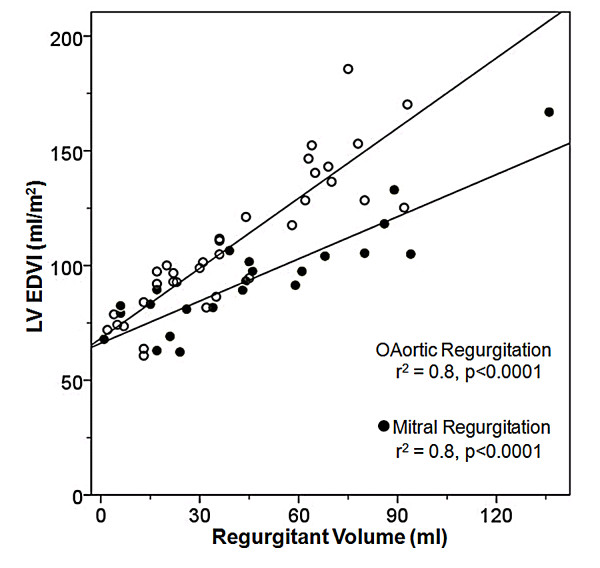
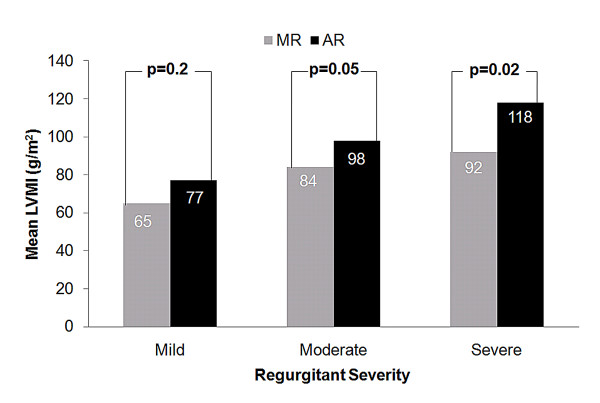
Results: There is a strong, linear relationship between regurgitant volume and LV end-diastolic volume index (aortic regurgitation r2 = 0.8, mitral regurgitation r2 = 0.8). Bland-Altman analysis of regurgitant volume shows little interobserver variation (AR: 0.6 +/- 4 ml; MR 4 +/- 6 ml). The correlation is much poorer between regurgitant volume and commonly used clinical linear measures such as end-systolic dimension (mitral regurgitation r2 = 0.3, aortic regurgitation r2 = 0.5). For a given regurgitant volume, AR causes greater LV enlargement and hypertrophy than MR.
Conclusion: CMR is an accurate and robust technique for quantifying regurgitant volume in patients with AR or MR. Ventricular volumes show a stronger correlation with regurgitant volume than linear dimensions, suggesting LV volumes better reflect ventricular remodeling in patients with isolated mitral or aortic regurgitation. Ventricular volumes that correspond to published recommended linear dimensions are determined to guide the timing of surgical intervention.
Figures
Comment in
-
Left Ventricular Size Is Critical for the Echocardiographic Assessment of Chronic Severe Mitral Regurgitation.J Am Coll Cardiol. 2015 Sep 29;66(13):1519-21. doi: 10.1016/j.jacc.2015.05.084. J Am Coll Cardiol. 2015. PMID: 26403350 No abstract available.
-
Reply: Left Ventricular Size Is Critical for the Echocardiographic Assessment of Chronic Severe Mitral Regurgitation.J Am Coll Cardiol. 2015 Sep 29;66(13):1521. doi: 10.1016/j.jacc.2015.06.1341. J Am Coll Cardiol. 2015. PMID: 26403352 No abstract available.
References
-
- Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52(13):e1–142. doi: 10.1016/j.jacc.2008.05.007. - DOI - PubMed
-
- Wittlinger T, Dzemali O, Bakhtiary F, Moritz A, Kleine P. Hemodynamic evaluation of aortic regurgitation by magnetic resonance imaging. Asian Cardiovasc Thorac Ann. 2008;16(4):278–283. - PubMed
-
- Dulce MC, Mostbeck GH, O'Sullivan M, Cheitlin M, Caputo GR, Higgins CB. Severity of aortic regurgitation: interstudy reproducibility of measurements with velocity-encoded cine MR imaging. Radiology. 1992;185(1):235–240. - PubMed
-
- Hundley WG, Li HF, Willard JE, Landau C, Lange RA, Meshack BM, Hillis LD, Peshock RM. Magnetic resonance imaging assessment of the severity of mitral regurgitation. Comparison with invasive techniques. Circulation. 1995;92(5):1151–1158. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
