

Prospects for mTOR inhibitor use in patients with polycystic kidney disease and hamartomatous diseases
- PMID: 20498248
- PMCID: PMC5619657
- DOI: 10.2215/CJN.01360210
Prospects for mTOR inhibitor use in patients with polycystic kidney disease and hamartomatous diseases
Abstract
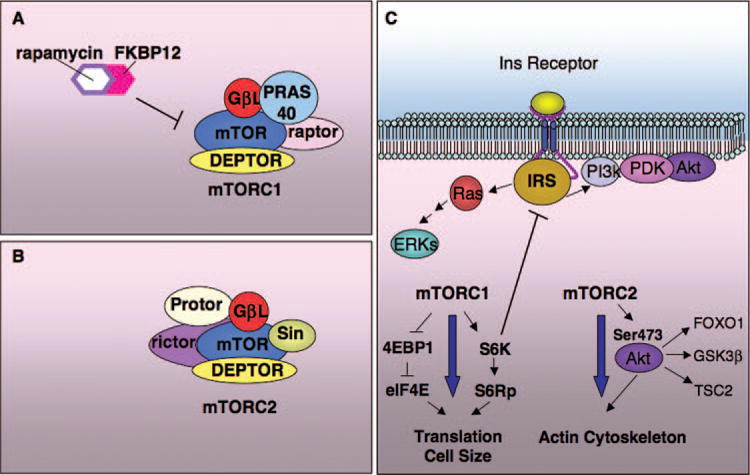
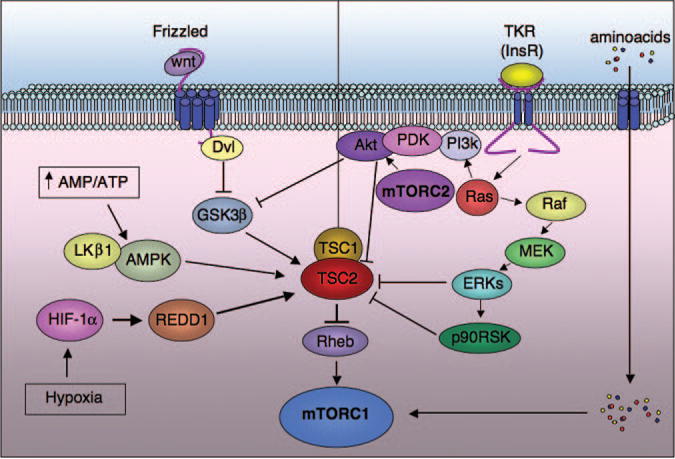
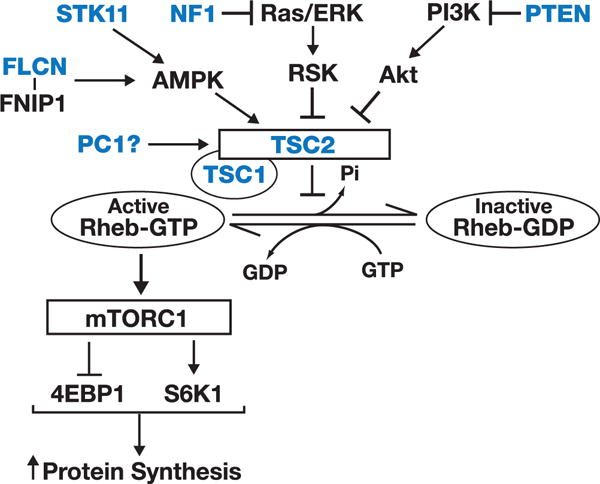
Mammalian target of rapamycin (mTOR) is the core component of two complexes, mTORC1 and mTORC2. mTORC1 is inhibited by rapamycin and analogues. mTORC2 is impeded only in some cell types by prolonged exposure to these compounds. mTOR activation is linked to tubular cell proliferation in animal models and human autosomal dominant polycystic kidney disease (ADPKD). mTOR inhibitors impede cell proliferation and cyst growth in polycystic kidney disease (PKD) models. After renal transplantation, two small retrospective studies suggested that mTOR was more effective than calcineurin inhibitor-based immunosuppression in limiting kidney and/or liver enlargement. By inhibiting vascular remodeling, angiogenesis, and fibrogenesis, mTOR inhibitors may attenuate nephroangiosclerosis, cyst growth, and interstitial fibrosis. Thus, they may benefit ADPKD at multiple levels. However, mTOR inhibition is not without risks and side effects, mostly dose-dependent. Under certain conditions, mTOR inhibition interferes with adaptive increases in renal proliferation necessary for recovery from injury. They restrict Akt activation, nitric oxide synthesis, and endothelial cell survival (downstream from mTORC2) and potentially increase the risk for glomerular and peritubular capillary loss, vasospasm, and hypertension. They impair podocyte integrity pathways and may predispose to glomerular injury. Administration of mTOR inhibitors is discontinued because of side effects in up to 40% of transplant recipients. Currently, treatment with mTOR inhibitors should not be recommended to treat ADPKD. Results of ongoing studies must be awaited and patients informed accordingly. If effective, lower dosages than those used to prevent rejection would minimize side effects. Combination therapy with other effective drugs could improve tolerability and results.
Figures
Similar articles
-
An mTOR kinase inhibitor slows disease progression in a rat model of polycystic kidney disease.Nephrol Dial Transplant. 2015 Jan;30(1):45-53. doi: 10.1093/ndt/gfu296. Epub 2014 Sep 19. Nephrol Dial Transplant. 2015. PMID: 25239638 Free PMC article.
-
A study of sirolimus and mTOR kinase inhibitor in a hypomorphic Pkd1 mouse model of autosomal dominant polycystic kidney disease.Am J Physiol Renal Physiol. 2019 Jul 1;317(1):F187-F196. doi: 10.1152/ajprenal.00051.2019. Epub 2019 May 1. Am J Physiol Renal Physiol. 2019. PMID: 31042058 Free PMC article.
-
An mTOR anti-sense oligonucleotide decreases polycystic kidney disease in mice with a targeted mutation in Pkd2.Hum Mol Genet. 2014 Sep 15;23(18):4919-31. doi: 10.1093/hmg/ddu208. Epub 2014 May 8. Hum Mol Genet. 2014. PMID: 24847003 Free PMC article.
-
Dissecting the role of mTOR: lessons from mTOR inhibitors.Biochim Biophys Acta. 2010 Mar;1804(3):433-9. doi: 10.1016/j.bbapap.2009.12.001. Epub 2009 Dec 11. Biochim Biophys Acta. 2010. PMID: 20005306 Review.
-
mTOR Signaling in Kidney Diseases.Kidney360. 2020 Sep 3;1(11):1319-1327. doi: 10.34067/KID.0003782020. eCollection 2020 Nov 25. Kidney360. 2020. PMID: 35372878 Free PMC article. Review.
Cited by
-
Bicaudal C mutation causes myc and TOR pathway up-regulation and polycystic kidney disease-like phenotypes in Drosophila.PLoS Genet. 2017 Apr 13;13(4):e1006694. doi: 10.1371/journal.pgen.1006694. eCollection 2017 Apr. PLoS Genet. 2017. PMID: 28406902 Free PMC article.
-
Advances and Challenges in Modeling Autosomal Dominant Polycystic Kidney Disease: A Focus on Kidney Organoids.Biomedicines. 2025 Feb 19;13(2):523. doi: 10.3390/biomedicines13020523. Biomedicines. 2025. PMID: 40002937 Free PMC article. Review.
-
Hypertension and Prohypertensive Antineoplastic Therapies in Cancer Patients.Circ Res. 2021 Apr 2;128(7):1040-1061. doi: 10.1161/CIRCRESAHA.121.318051. Epub 2021 Apr 1. Circ Res. 2021. PMID: 33793337 Free PMC article. Review.
-
Efficient protocol for the differentiation of kidney podocytes from induced pluripotent stem cells, involving the inhibition of mTOR.Sci Rep. 2023 Nov 16;13(1):20010. doi: 10.1038/s41598-023-47087-8. Sci Rep. 2023. PMID: 37973990 Free PMC article.
-
Management of autosomal-dominant polycystic kidney disease-state-of-the-art.Clin Kidney J. 2018 Dec;11(Suppl 1):i2-i13. doi: 10.1093/ckj/sfy103. Epub 2018 Dec 17. Clin Kidney J. 2018. PMID: 30581561 Free PMC article. Review.
References
-
- Torres VE, Harris PC, Pirson Y. Autosomal dominant polycystic kidney disease. Lancet. 2007;369:1287–1301. - PubMed
-
- Roach ES, Gomez MR, Northrup H. Tuberous sclerosis complex consensus conference: Revised clinical diagnostic criteria. J Child Neurol. 1998;13:624–628. - PubMed
-
- European Chromosome 16 Tuberous Sclerosis Consortium. Identification and characterization of the tuberous sclerosis gene on chromosome 16. Cell. 1993;75:1305–1315. - PubMed
-
- The European Polycystic Kidney Disease Consortium. The polycystic kidney disease 1 gene encodes a 14 kb transcript and lies within a duplicated region on chromosome 16. Cell. 1994;78:725. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
