

Sleep disturbance and melatonin levels following traumatic brain injury
- PMID: 20498441
- PMCID: PMC3462582
- DOI: 10.1212/WNL.0b013e3181e0438b
Sleep disturbance and melatonin levels following traumatic brain injury
Abstract
Objectives: Sleep disturbances commonly follow traumatic brain injury (TBI) and contribute to ongoing disability. However, there are no conclusive findings regarding specific changes to sleep quality and sleep architecture measured using polysomnography. Possible causes of the sleep disturbances include disruption of circadian regulation of sleep-wakefulness, psychological distress, and a neuronal response to injury. We investigated sleep-wake disturbances and their underlying mechanisms in a TBI patient sample.
Methods: This was an observational study comparing 23 patients with TBI (429.7 +/- 287.6 days post injury) and 23 age- and gender-matched healthy volunteers on polysomnographic sleep measures, salivary dim light melatonin onset (DLMO) time, and self-reported sleep quality, anxiety, and depression.
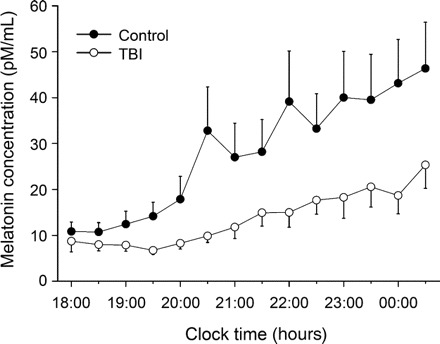
Results: Patients with TBI reported higher anxiety and depressive symptoms and sleep disturbance than controls. Patients with TBI showed decreased sleep efficiency (SE) and increased wake after sleep onset (WASO). Although no significant group differences were found in sleep architecture, when anxiety and depression scores were controlled, patients with TBI showed higher amount of slow wave sleep. No differences in self-reported sleep timing or salivary DLMO time were found. However, patients with TBI showed significantly lower levels of evening melatonin production. Melatonin level was significantly correlated with REM sleep but not SE or WASO.
Conclusions: Reduced evening melatonin production may indicate disruption to circadian regulation of melatonin synthesis. The results suggest that there are at least 2 factors contributing to sleep disturbances in patients with traumatic brain injury. We propose that elevated depression is associated with reduced sleep quality, and increased slow wave sleep is attributed to the effects of mechanical brain damage.
Figures
Similar articles
-
Circadian Melatonin Rhythm Following Traumatic Brain Injury.Neurorehabil Neural Repair. 2016 Nov;30(10):972-977. doi: 10.1177/1545968316650279. Epub 2016 May 23. Neurorehabil Neural Repair. 2016. PMID: 27221043
-
Assessing Sleep Architecture With Polysomnography During Posttraumatic Amnesia After Traumatic Brain Injury: A Pilot Study.Neurorehabil Neural Repair. 2021 Jul;35(7):622-633. doi: 10.1177/15459683211011241. Epub 2021 May 12. Neurorehabil Neural Repair. 2021. PMID: 33978535
-
Sleep Disturbance During Post-Traumatic Amnesia and Early Recovery After Traumatic Brain Injury.J Neurotrauma. 2024 Aug;41(15-16):e1961-e1975. doi: 10.1089/neu.2023.0656. Epub 2024 May 6. J Neurotrauma. 2024. PMID: 38553904
-
Fatigue and sleep disturbance following traumatic brain injury--their nature, causes, and potential treatments.J Head Trauma Rehabil. 2012 May-Jun;27(3):224-33. doi: 10.1097/HTR.0b013e31824ee1a8. J Head Trauma Rehabil. 2012. PMID: 22573041 Review.
-
The Utility of Melatonin for the Treatment of Sleep Disturbance After Traumatic Brain Injury: A Scoping Review.Arch Phys Med Rehabil. 2023 Feb;104(2):340-349. doi: 10.1016/j.apmr.2022.09.018. Epub 2022 Oct 13. Arch Phys Med Rehabil. 2023. PMID: 36243124
Cited by
-
Altered sleep composition after traumatic brain injury does not affect declarative sleep-dependent memory consolidation.Front Hum Neurosci. 2015 Jun 5;9:328. doi: 10.3389/fnhum.2015.00328. eCollection 2015. Front Hum Neurosci. 2015. PMID: 26097451 Free PMC article.
-
Traumatic brain injury and sleep disorders.Neurol Clin. 2012 Nov;30(4):1299-312. doi: 10.1016/j.ncl.2012.08.008. Neurol Clin. 2012. PMID: 23099139 Free PMC article. Review.
-
Traumatic Optic Neuropathy Is Associated with Visual Impairment, Neurodegeneration, and Endoplasmic Reticulum Stress in Adolescent Mice.Cells. 2021 Apr 23;10(5):996. doi: 10.3390/cells10050996. Cells. 2021. PMID: 33922788 Free PMC article.
-
Salivary Biomarkers as Indicators of TBI Diagnosis and Prognosis: A Systematic Review.Mol Diagn Ther. 2022 Mar;26(2):169-187. doi: 10.1007/s40291-021-00569-9. Epub 2022 Jan 20. Mol Diagn Ther. 2022. PMID: 35048328
-
Circadian therapy interventions for glymphatic dysfunction in concussions injuries: A narrative review.Sci Prog. 2023 Jul-Sep;106(3):368504231189536. doi: 10.1177/00368504231189536. Sci Prog. 2023. PMID: 37499049 Free PMC article. Review.
References
-
- Baumann CR, Werth E, Stocker R, Ludwig S, Bassetti CL. Sleep-wake disturbances 6 months after traumatic brain injury: a prospective study. Brain 2007;130:1873–1883. - PubMed
-
- Clinchot DM, Bogner J, Mysiw WJ, Fugate L, Corrigan J. Defining sleep disturbance after brain injury. Am J Phys Med Rehabil 1998;77:291–295. - PubMed
-
- Hibbard MR, Uysal S, Sliwinski M, Gordon WA. Undiagnosed health issues in individuals with traumatic brain injury living in the community. J Head Trauma Rehabil 1998;13:47–57. - PubMed
-
- Makley MJ, English JB, Drubach DA, Kreuz AJ, Celnik PA, Tarwater PM. Prevalence of sleep disturbance in closed head injury patients in a rehabilitation unit. Neurorehabil Neural Repair 2008;22:341–347. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical