

Long-term outcomes in patients with high-risk myeloid malignancies following matched related donor hematopoietic cell transplantation with myeloablative conditioning of BU, etoposide and CY
- PMID: 20498648
- PMCID: PMC4466222
- DOI: 10.1038/bmt.2010.114
Long-term outcomes in patients with high-risk myeloid malignancies following matched related donor hematopoietic cell transplantation with myeloablative conditioning of BU, etoposide and CY
Abstract
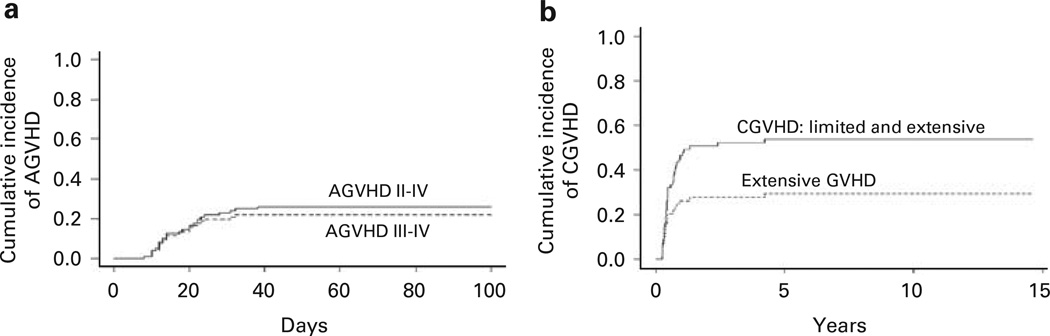
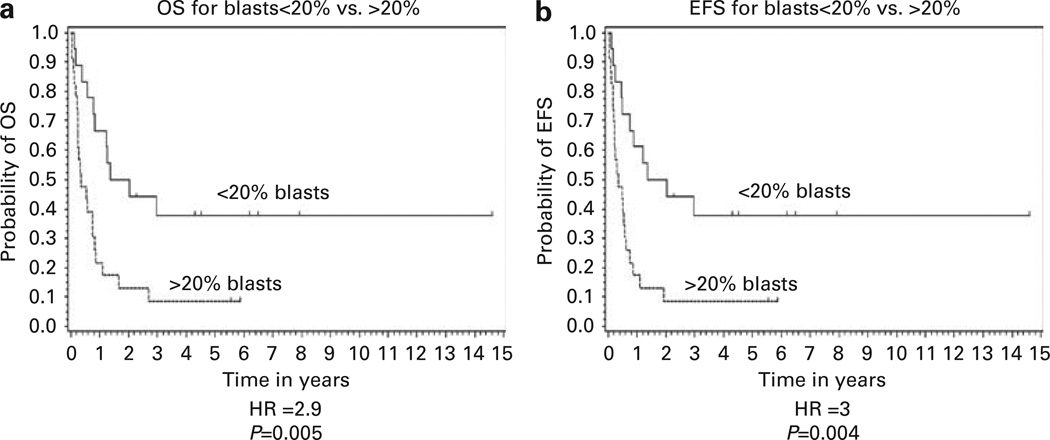
Patients with high-risk or advanced myeloid malignancies have limited effective treatment options. These include high-dose therapy followed by allogeneic hematopoietic cell transplantation (HCT). We report a single-institution, long-term follow-up of 96 patients, median age 50 (range, 20-60) years, who received HLA-matched related HCT between 1992 and 2007. All patients were treated with a uniform preparatory regimen intended to enhance the widely used regimen of BU and CY that included: BU 16.0 mg/kg (days -8 to -5), etoposide 60 mg/kg (day -4), CY 60 mg/kg (day -2) with GVHD prophylaxis of CsA or FK506 and prednisone. Disease status at transplantation was high-risk AML (n=41), CML in second chronic phase or blast crisis (n=8), myelofibrosis and myeloproliferative disorders (n=8), and myelodysplasia (n=39). Thirty-six percent (n=35) of patients received BM whereas 64% (n=61) received G-CSF-mobilized PBPC. With a median follow-up of 5.6 years (range, 1.6-14.6 years) actuarial 5-year OS was 32% (95% CI 22-42) and 5-year EFS was 31% (95% CI 21-41). Relapse rate was 24% (95% CI 15-33) at 2 and 5 years. Nonrelapse mortality was 29% (95% CI 20-38) at day 100 and 38% (95% CI 29-47) at 1 year. Cumulative incidence of acute (grade II-IV) and extensive chronic GVHD was 27% (95% CI 18-36) and 29% (95% CI 18-40), respectively. There was no statistically significant difference in OS (31 vs 32%, P=0.89) or relapse rates (17 vs 28%, P=0.22) for recipients of BM vs PBPC, respectively. These results confirm that patients with high-risk or advanced myeloid malignancies can achieve long-term survival following myeloablative allogeneic HCT with aggressive conditioning.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
A Phase I study of gemtuzumab ozogamicin (GO) in combination with busulfan and cyclophosphamide (Bu/Cy) and allogeneic stem cell transplantation in children with poor-risk CD33+ AML: a new targeted immunochemotherapy myeloablative conditioning (MAC) regimen.Biol Blood Marrow Transplant. 2012 Feb;18(2):324-9. doi: 10.1016/j.bbmt.2011.11.007. Epub 2011 Nov 9. Biol Blood Marrow Transplant. 2012. PMID: 22079471 Clinical Trial.
-
Comparison of total body irradiation vs busulfan in combination with cyclophosphamide as conditioning for unrelated stem cell transplantation in CML patients.Bone Marrow Transplant. 2001 Feb;27(4):349-54. doi: 10.1038/sj.bmt.1702802. Bone Marrow Transplant. 2001. PMID: 11313663 Clinical Trial.
-
[A comparison of toxicity and efficacy between busulfan plus fludarabine and busulfan plus cyclophosphamide for allogeneic hematopoietic stem cell transplantation in acute myeloid leukemia].Zhonghua Nei Ke Za Zhi. 2012 Nov;51(11):880-4. Zhonghua Nei Ke Za Zhi. 2012. PMID: 23291027 Chinese.
-
Allogeneic hematopoietic stem-cell transplantation for acute myeloid leukemia in remission: comparison of intravenous busulfan plus cyclophosphamide (Cy) versus total-body irradiation plus Cy as conditioning regimen--a report from the acute leukemia working party of the European group for blood and marrow transplantation.J Clin Oncol. 2013 Oct 1;31(28):3549-56. doi: 10.1200/JCO.2013.48.8114. Epub 2013 Aug 26. J Clin Oncol. 2013. PMID: 23980086
-
Comparative effectiveness of busulfan/cyclophosphamide versus busulfan/fludarabine myeloablative conditioning for allogeneic hematopoietic cell transplantation in acute myeloid leukemia and myelodysplastic syndrome.Hematol Oncol Stem Cell Ther. 2020 Sep;13(3):160-165. doi: 10.1016/j.hemonc.2019.09.002. Epub 2019 Oct 11. Hematol Oncol Stem Cell Ther. 2020. PMID: 31628924 Clinical Trial.
Cited by
-
Sirolimus and mycophenolate mofetil as GVHD prophylaxis in myeloablative, matched-related donor hematopoietic cell transplantation.Bone Marrow Transplant. 2012 Apr;47(4):581-8. doi: 10.1038/bmt.2011.104. Epub 2011 May 9. Bone Marrow Transplant. 2012. PMID: 21552302 Free PMC article.
-
Allogeneic hematopoietic cell transplant for normal karyotype AML: indirect evidence of selection for adverse molecular profile.Bone Marrow Transplant. 2015 Jul;50(7):1004-1006. doi: 10.1038/bmt.2015.62. Epub 2015 Apr 20. Bone Marrow Transplant. 2015. PMID: 25893457 Free PMC article. No abstract available.
-
Busulphan-cyclophosphamide cause endothelial injury, remodeling of resistance arteries and enhanced expression of endothelial nitric oxide synthase.PLoS One. 2012;7(1):e30897. doi: 10.1371/journal.pone.0030897. Epub 2012 Jan 27. PLoS One. 2012. PMID: 22303468 Free PMC article.
-
Pretransplantation use of the second-generation tyrosine kinase inhibitors has no negative impact on the HCT outcome.Ann Hematol. 2015 Nov;94(11):1891-7. doi: 10.1007/s00277-015-2457-1. Epub 2015 Jul 29. Ann Hematol. 2015. PMID: 26220759 Free PMC article.
References
-
- Fung HC, Stein A, Slovak M, O’Donnell MR, Snyder DS, Cohen S, et al. A long-term follow-up report on allogeneic stem cell transplantation for patients with primary refractory acute myelogenous leukemia: impact of cytogenetic characteristics on transplantation outcome. Biol Blood Marrow Transplant. 2003;9:766–771. - PubMed
-
- Appelbaum FR, Clift RA, Buckner CD, Stewart P, Storb R, Sullivan KM, et al. Allogeneic marrow transplantation for acute nonlymphoblastic leukemia after first relapse. Blood. 1983;61:949–953. - PubMed
-
- Gale RP, Horowitz MM, Rees JK, Gray RG, Oken MM, Estey EH, et al. Chemotherapy versus transplants for acute myelogenous leukemia in second remission. Leukemia. 1996;10:13–19. - PubMed
-
- Kebriaei P, Kline J, Stock W, Kasza K, Le Beau MM, Larson RA, et al. Impact of disease burden at time of allogeneic stem cell transplantation in adults with acute myeloid leukemia and myelodysplastic syndromes. Bone Marrow Transplant. 2005;35:965–970. - PubMed
-
- Wong R, Shahjahan M, Wang X, Thall PF, De Lima M, Khouri I, et al. Prognostic factors for outcomes of patients with refractory or relapsed acute myelogenous leukemia or myelodysplastic syndromes undergoing allogeneic progenitor cell transplantation. Biol Blood Marrow Transplant. 2005;11:108–114. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
