

Statin-associated muscle-related adverse effects: a case series of 354 patients
- PMID: 20500044
- PMCID: PMC4729295
- DOI: 10.1592/phco.30.6.541
Statin-associated muscle-related adverse effects: a case series of 354 patients
Abstract
Study objective: To characterize the properties and natural history of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor (statin)-associated muscle-related adverse effects (MAEs).
Design: Patient-targeted postmarketing adverse-effect surveillance approach coupling survey design with an open-ended narrative.
Setting: University-affiliated health care system.
Subjects: Three hundred fifty-four patients (age range 34-86 yrs) who self-reported muscle-related problems associated with statin therapy.
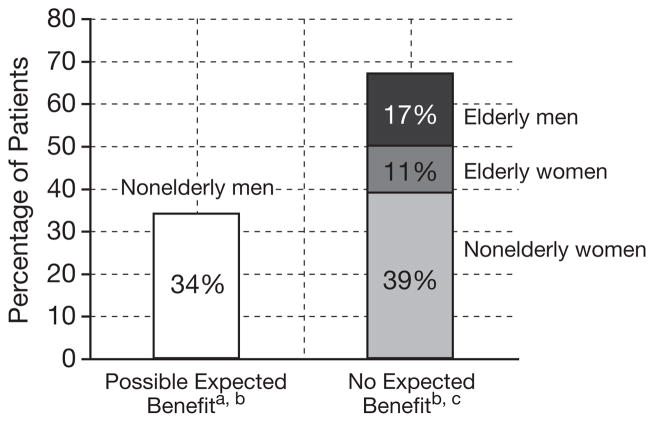
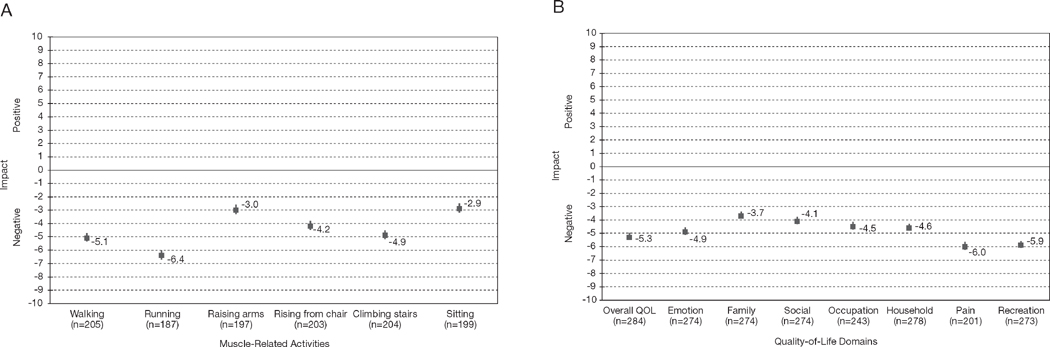
Measurements and main results: Patients with perceived statin-associated MAEs completed a survey assessing statin drugs and dosages; characteristics of the MAEs; time course of onset, resolution, or recurrence; and impact on quality of life (QOL). Cases were assessed for putative drug adverse-effect causality by using the Naranjo adverse drug reaction probability scale criteria and were evaluated for inclusion in groups for which mortality benefit with statins has been shown. Patients reported muscle pain (93%), fatigue (88%), and weakness (85%). Three hundred patients (85%) met literature criteria for probable or definite drug adverse-effect causality. Ninety-four percent of atorvastatin usages (240/255) generated MAEs versus 61% of lovastatin usages (38/62, p<0.0001). Higher potency statins reproduced MAEs in 100% of 39 rechallenges versus 73% (29/40) with lower potency rechallenges (p<0.01). Time course of onset after statin initiation varied (median 14 wks); some MAEs occurred after long-term symptom-free use. Recurrence with rechallenge had a significantly shorter latency to onset (median 2 wks). The MAEs adversely affected all assessed functional and QOL domains. Most patients with probable or definite MAEs were in categories for which available randomized controlled trial evidence shows no trend to all-cause mortality benefit with statin therapy.
Conclusion: This study complements available information on the properties and natural history of statin-associated MAEs, affirming dose dependence and strong QOL impact. The data indicating a dose-dependent relationship between MAE risk and recurrence suggest lower potency statins or discontinuation may bear consideration for ameliorating symptoms.
Figures
References
-
- IMS Health. [Accessed April 19, 2002];US top ten products by prescriptions. Available from http://wwwimshealthcom/public/structure/dispcontent/1,2779,1343-1343-144....
-
- IMS Health. [Accessed May 23, 2005];Lipitor leads the way in 2003. Available from http://wwwims-globalcom/insight/news_story/0403/news_story_040316htm.
-
- IMS Health. [Accessed May 2, 2008];IMS global insights – IMS retail drug monitor. 2007 Dec; Available from http://wwwimshealthcom/web/content/0,3148,64576068_63872702_70260998_837....
-
- Scott RS, Lintott CJ, Wilson MJ. Simvastatin and side effects. N Z Med J. 1991;104:493–5. - PubMed
-
- Wierzbicki AS, Lumb PJ, Semra Y, Chik G, Christ ER, Crook MA. Atorvastatin compared with simvastatin-based therapies in the management of severe familial hyperlipidaemias. QJM. 1999;92:387–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous