

Primary hemiarthroplasty versus conservative treatment for comminuted fractures of the proximal humerus in the elderly (ProCon): a multicenter randomized controlled trial
- PMID: 20500849
- PMCID: PMC2887776
- DOI: 10.1186/1471-2474-11-97
Primary hemiarthroplasty versus conservative treatment for comminuted fractures of the proximal humerus in the elderly (ProCon): a multicenter randomized controlled trial
Abstract
Background: Fractures of the proximal humerus are associated with a profound temporary and sometimes permanent, impairment of function and quality of life. The treatment of comminuted fractures of the proximal humerus like selected three-or four-part fractures and split fractures of the humeral head is a demanding and unresolved problem, especially in the elderly. Locking plates appear to offer improved fixation; however, screw cut-out rates ranges due to fracture collapse are high. As this may lead to higher rates of revision surgery, it may be preferable to treat comminuted fractures in the elderly primarily with a prosthesis or non-operatively. Results from case series and a small-sample randomized controlled trial (RCT) suggest improved function and less pain after primary hemiarthroplasty (HA); however these studies had some limitations and a RCT is needed. The primary aim of this study is to compare the Constant scores (reflecting functional outcome and pain) at one year after primary HA versus non-operative treatment in elderly patients who sustained a comminuted proximal humeral fracture. Secondary aims include effects on functional outcome, pain, complications, quality of life, and cost-effectiveness.
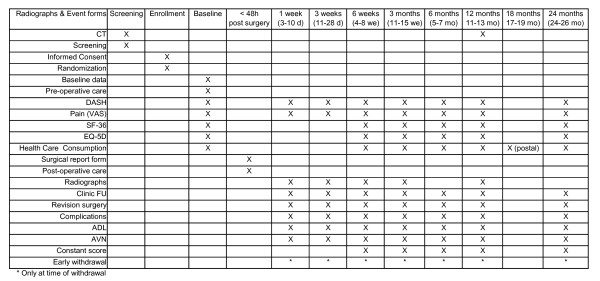
Methods/design: A prospective, multi-center RCT will be conducted in nine centers in the Netherlands and Belgium. Eighty patients over 65 years of age, who have sustained a three-or four part, or split head proximal humeral fracture will be randomized between primary hemiarthroplasty and conservative treatment. The primary outcome is the Constant score, which indicates pain and function. Secondary outcomes include the Disability of the Arm and Shoulder (DASH) score, Visual Analogue Scale (VAS) for pain, radiographic healing, health-related quality of life (Short-form-36, EuroQol-5D) and healthcare consumption. Cost-effectiveness ratios will be determined for both trial arms. Outcome will be monitored at regular intervals over the subsequent 24 months (1, 3 and 6 weeks, and 3, 6, 12, 18, and 24 months). Data will be analyzed on an intention to treat basis, using univariate and multivariable analyses.
Discussion: This trial will provide level-1 evidence on the effectiveness of the two mostly applied treatment options for three-or four part and split head proximal humeral fractures in the elderly. These data may support the development of a clinical guideline for treatment of these traumatic injuries.
Trial registration: Netherlands Trial Register (NTR2040).
Figures
References
-
- Handoll HH, Gibson JN, Madhok R. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev. 2003. p. CD000434. - PubMed
-
- Lill H, Hepp P, Korner J, Kassi JP, Verheyden AP, Josten C, Duda GN. Proximal humeral fractures: how stiff should an implant be? A comparative mechanical study with new implants in human specimens. Arch Orthop Trauma Surg. 2003;123:74–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
