

Summary of data reported to CDC's national automated biosurveillance system, 2008
- PMID: 20500863
- PMCID: PMC2890598
- DOI: 10.1186/1472-6947-10-30
Summary of data reported to CDC's national automated biosurveillance system, 2008
Abstract
Background: BioSense is the US national automated biosurveillance system. Data regarding chief complaints and diagnoses are automatically pre-processed into 11 broader syndromes (e.g., respiratory) and 78 narrower sub-syndromes (e.g., asthma). The objectives of this report are to present the types of illness and injury that can be studied using these data and the frequency of visits for the syndromes and sub-syndromes in the various data types; this information will facilitate use of the system and comparison with other systems.
Methods: For each major data source, we summarized information on the facilities, timeliness, patient demographics, and rates of visits for each syndrome and sub-syndrome.
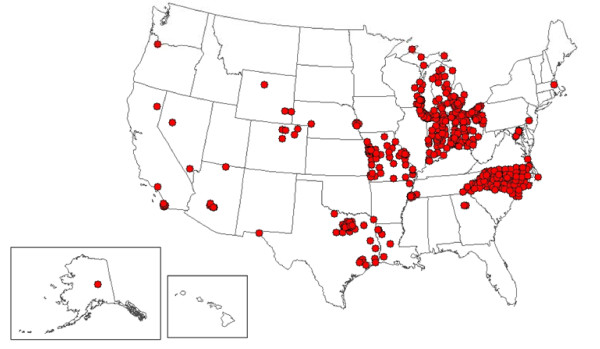
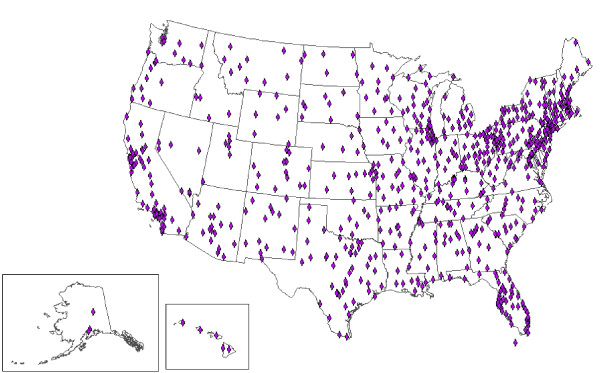
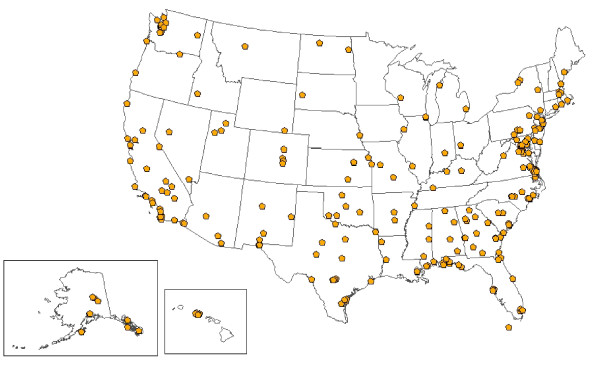
Results: In 2008, the primary data sources were the 333 US Department of Defense, 770 US Veterans Affairs, and 532 civilian hospital emergency department facilities. Median times from patient visit to record receipt at CDC were 2.2 days, 2.0 days, and 4 hours for these sources respectively. Among sub-syndromes, we summarize mean 2008 visit rates in 45 infectious disease categories, 11 injury categories, 7 chronic disease categories, and 15 other categories.
Conclusions: We present a systematic summary of data that is automatically available to public health departments for monitoring and responding to emergencies.
Figures
References
-
- Buehler JW, Sonricker A, Paladine M, Soper P, Mostashari F. Syndromic surveillance practice in the United States: findings from a survey of state, territorial, and selected local health departments. Advances in Disease Surveillance. 2008;6:1–8.
MeSH terms
LinkOut - more resources
Full Text Sources
