

Which mesh for hernia repair?
- PMID: 20501011
- PMCID: PMC3025220
- DOI: 10.1308/003588410X12664192076296
Which mesh for hernia repair?
Abstract
Introduction: The concept of using a mesh to repair hernias was introduced over 50 years ago. Mesh repair is now standard in most countries and widely accepted as superior to primary suture repair. As a result, there has been a rapid growth in the variety of meshes available and choosing the appropriate one can be difficult. This article outlines the general properties of meshes and factors to be considered when selecting one.
Materials and methods: We performed a search of the medical literature from 1950 to 1 May 2009, as indexed by Medline, using the PubMed search engine (www.pubmed.gov). To capture all potentially relevant articles with the highest degree of sensitivity, the search terms were intentionally broad. We used the following terms: 'mesh, pore size, strength, recurrence, complications, lightweight, properties'. We also hand-searched the bibliographies of relevant articles and product literature to identify additional pertinent reports.
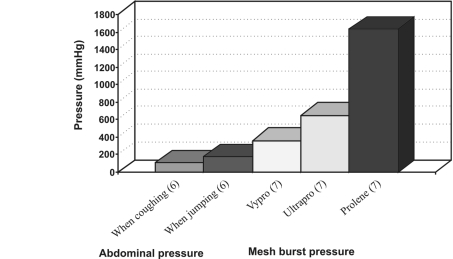
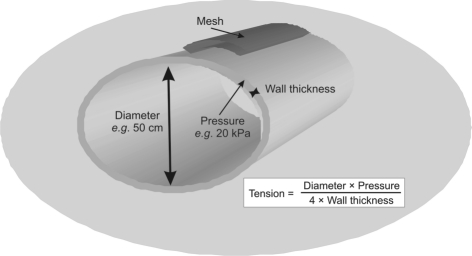
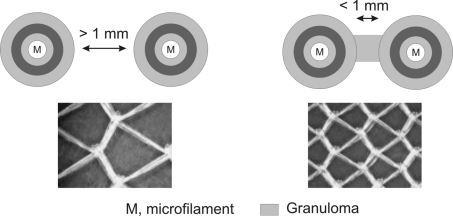
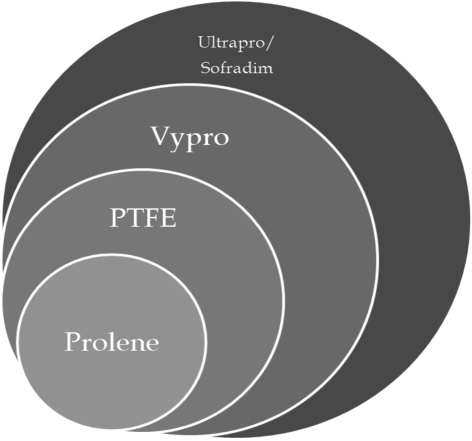
Results and conclusions: The most important properties of meshes were found to be the type of filament, tensile strength and porosity. These determine the weight of the mesh and its biocompatibility. The tensile strength required is much less than originally presumed and light-weight meshes are thought to be superior due to their increased flexibility and reduction in discomfort. Large pores are also associated with a reduced risk of infection and shrinkage. For meshes placed in the peritoneal cavity, consideration should also be given to the risk of adhesion formation. A variety of composite meshes have been promoted to address this, but none appears superior to the others. Finally, biomaterials such as acellular dermis have a place for use in infected fields but have yet to prove their worth in routine hernia repair.
Figures
References
-
- Klinge U, Klosterhalfen B, Birkenhauer V, Junge K, Conze J, Schumpelick V. Impact of polymer pore size on the interface scar formation in a rat model. J Surg Res. 2002;103:208–14. - PubMed
-
- Nixon SJ, Jawaid H. Recurrence after inguinal hernia repair at ten years by open darn, open mesh and TEP – no advantage with mesh. Surgeon. 2009;7:71–4. - PubMed
-
- Klinge U. Mesh for hernia repair. Br J Surg. 2008;95:539–40. - PubMed
-
- O'Dwyer, Kingsworth AN, Molloy RG, Small PK, Lammers B, Horeyseck G. Randomized clinical trial assessing impact of a lightweight or heavyweight mesh on chronic pain after inguinal hernia repair. Br J Surg. 2005;92:166–70. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources