

Ischaemic nephropathy secondary to atherosclerotic renal artery stenosis: clinical and histopathological correlates
- PMID: 20501460
- PMCID: PMC2957590
- DOI: 10.1093/ndt/gfq269
Ischaemic nephropathy secondary to atherosclerotic renal artery stenosis: clinical and histopathological correlates
Abstract
Background: Advanced renal artery stenosis (RAS) may cause progressive deterioration in renal function. We correlated the histopathological findings and clinical characteristics in selected patients with atherosclerotic RAS who underwent nephrectomy of their small kidneys for resistant renovascular hypertension.
Methods: We studied 62 patients who underwent nephrectomy of a small kidney for uncontrolled hypertension between 1990 and 2000.
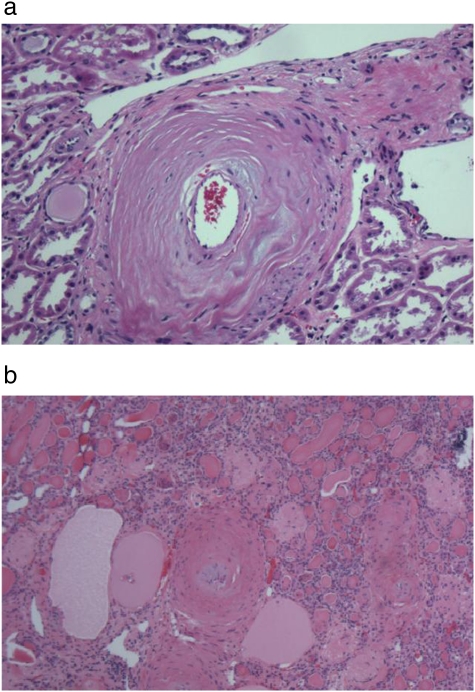
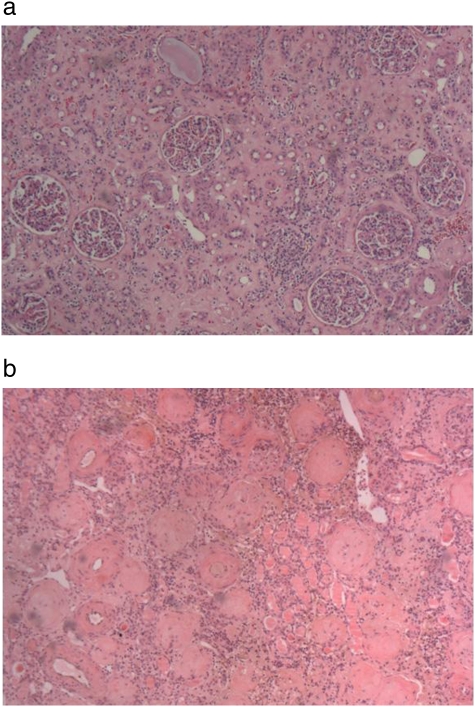
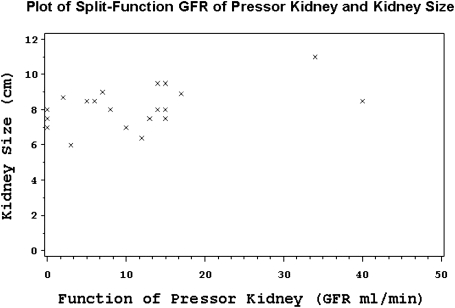
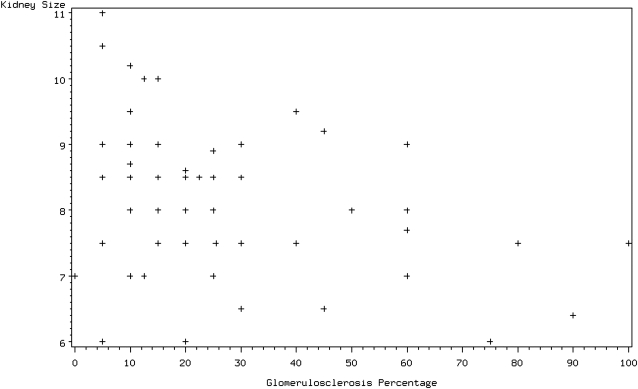
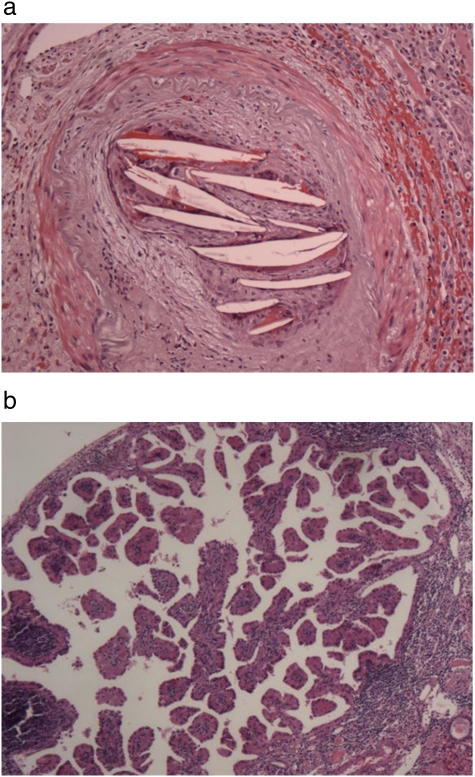
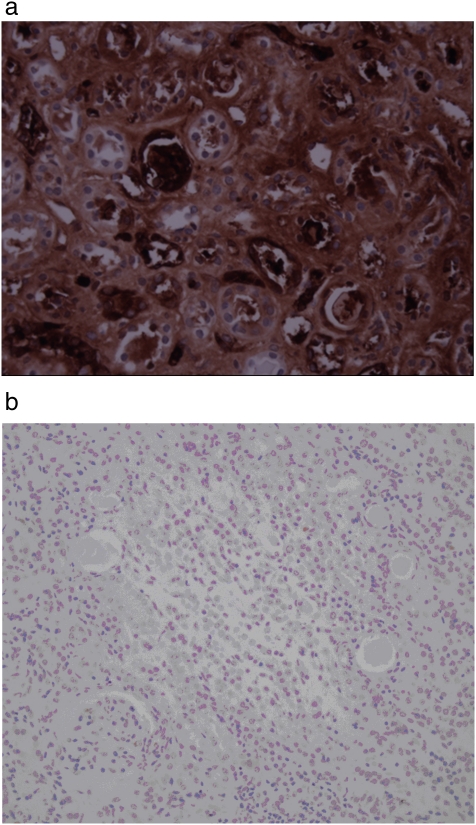
Results: The mean patient age was 65.4 ± 9.6 years; 28 (45%) were men. Significant tubulointerstitial atrophy with relative glomerular sparing was the predominant pattern of injury in 44 (71%) patients. In 14 (23%) patients, diffuse global glomerulosclerosis was present. The severity of tubulointerstitial atrophy and the extent of glomerulosclerosis were both associated with smaller kidney size (P = 0.002). Three patterns of vascular involvement were present: atheroembolic, atherosclerotic and hypertensive vascular changes, which were documented in 39, 98 and 52% of subjects, respectively. The presence and severity of these vascular changes positively correlated with both atherosclerotic risk factors, such as hypertension, dyslipidaemia and renal insufficiency, and cardiovascular morbidity, including abdominal aortic aneurysm and myocardial infarction. Patients on statin therapy were noted to have less evidence of renal fibrosis as measured by transforming growth factor-beta staining (P = 0.003).
Conclusion: The severity of renal histopathological findings in patients who underwent nephrectomy for resistant hypertension correlated with an increased prevalence of cardiovascular disease, a greater degree of renal dysfunction and more severe dyslipidaemia. Statin therapy may affect development of intra-renal injury by slowing the progression of fibrosis.
Figures
References
-
- Lerman L, Textor SC. Pathophysiology of ischemic nephropathy. Urol Clin North Am. 2001;28:793–803. - PubMed
-
- Textor SC, Wilcox CS. Renal artery stenosis: a common, treatable cause of renal failure? Annu Rev Med. 2001;52:421–442. - PubMed
-
- Guo H, Kalra PA, Gilbertson DT, et al. Atherosclerotic renovascular disease in older US patients starting dialysis, 1996 to 2001. Circulation. 2007;115:50–58. - PubMed
-
- Greco BA, Breyer JA. The natural history of renal artery stenosis: who should be evaluated for suspected ischemic nephropathy? Semin Nephrol. 1996;16:2–11. - PubMed
-
- Chade AR, Zhu XY, Grande JP, et al. Simvastatin abates development of renal fibrosis in experimental renovascular disease. J Hypertens. 2008;26:1651–1660. - PubMed
