

Chemoembolization for hepatocellular carcinoma: comprehensive imaging and survival analysis in a 172-patient cohort
- PMID: 20501733
- PMCID: PMC2948657
- DOI: 10.1148/radiol.10091473
Chemoembolization for hepatocellular carcinoma: comprehensive imaging and survival analysis in a 172-patient cohort
Abstract
Purpose: To determine comprehensive imaging and long-term survival outcome following chemoembolization for hepatocellular carcinoma (HCC).
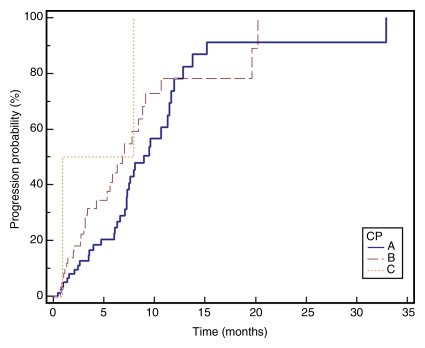
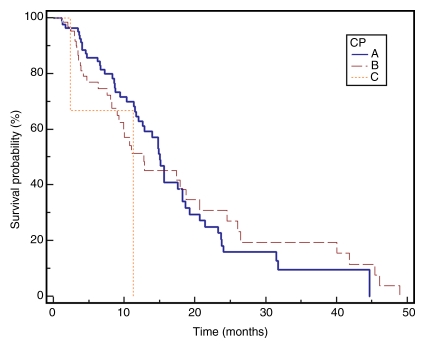
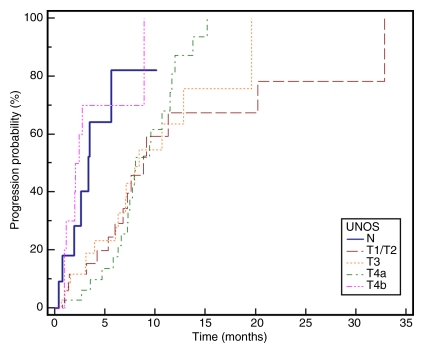
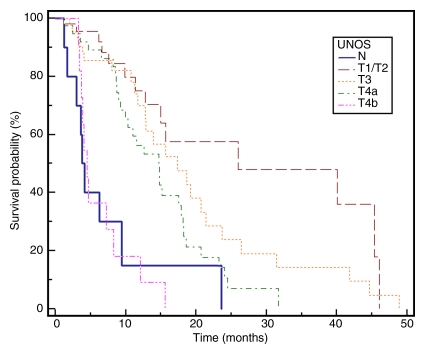
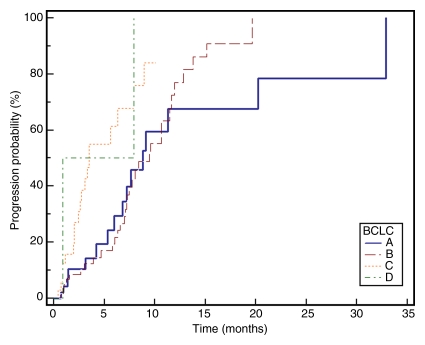
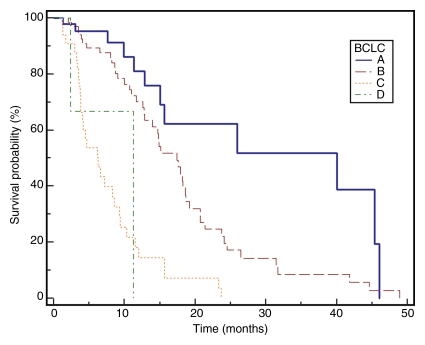
Materials and methods: One hundred seventy-two patients with HCC treated with chemoembolization were studied retrospectively in an institutional review board approved protocol; this study was HIPAA compliant. Baseline laboratory and imaging characteristics were obtained. Clinical and laboratory toxicities following treatment were assessed. Imaging characteristics following chemoembolization were evaluated to determine response rates (size and necrosis) and time to progression (TTP). Survival from the time of first chemoembolization treatment was calculated. Subanalyses were performed by stratifying the population according to Child-Pugh, United Network for Organ Sharing, and Barcelona Clinic for Liver Cancer (BCLC) staging systems.
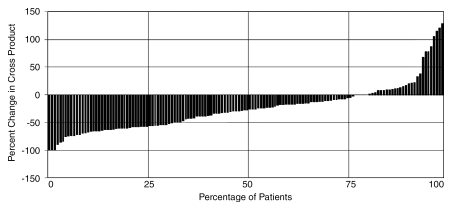
Results: Cirrhosis was present in 157 patients (91%); portal hypertension was present in 139 patients (81%). Eleven patients (6%) had metastases at baseline. Portal vein thrombosis was present in 11 patients (6%). Fifty-five percent of patients experienced some form of toxicity following treatment; 21% developed grade 3 or 4 bilirubin toxicity. Post-chemoembolization response was seen in 31% and 64% of patients according to size and necrosis criteria, respectively. Median TTP was 7.9 months (95% confidence interval: 7.1, 9.4) but varied widely by stage. Median survival was significantly different between patients with BCLC stages A, B, and C disease (stage A, 40.0 months; B, 17.4 months; C, 6.3 months; P < .0001).
Conclusion: The determination of TTP and survival in patients with HCC is confounded by tumor biology and background cirrhosis; chemoembolization was shown to be a safe and effective therapy in patients with HCC.
Copyright RSNA, 2010
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005;55(2):74–108 - PubMed
-
- Bosch FX, Ribes J, Díaz M, Cléries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology 2004;127(5 suppl 1):S5–S16 - PubMed
-
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996;334(11):693–699 - PubMed
-
- Kulik LM, Atassi B, van Holsbeeck L, et al. Yttrium-90 microspheres (TheraSphere) treatment of unresectable hepatocellular carcinoma: downstaging to resection, RFA and bridge to transplantation. J Surg Oncol 2006;94(7):572–586 - PubMed
-
- Lu DS, Yu NC, Raman SS, et al. Radiofrequency ablation of hepatocellular carcinoma: treatment success as defined by histologic examination of the explanted liver. Radiology 2005;234(3):954–960 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
