

Reversible epithelial to mesenchymal transition and acquired resistance to sunitinib in patients with renal cell carcinoma: evidence from a xenograft study
- PMID: 20501804
- PMCID: PMC3049816
- DOI: 10.1158/1535-7163.MCT-09-1106
Reversible epithelial to mesenchymal transition and acquired resistance to sunitinib in patients with renal cell carcinoma: evidence from a xenograft study
Abstract
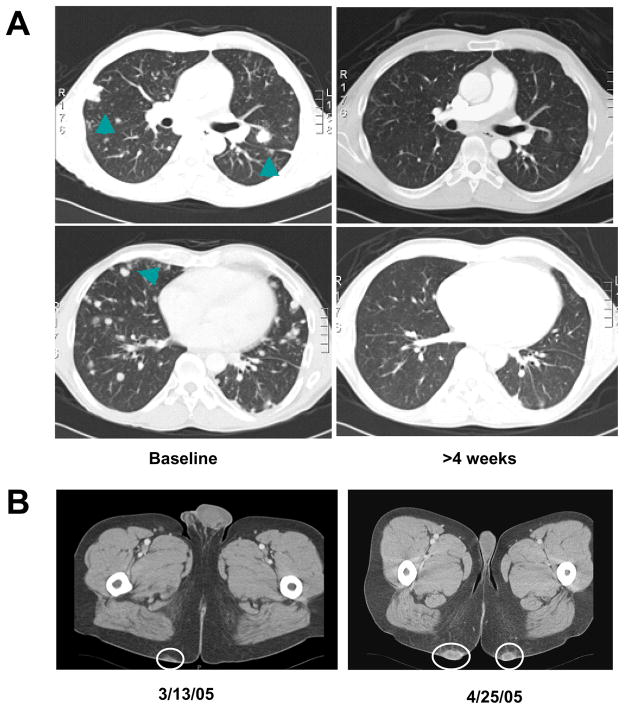
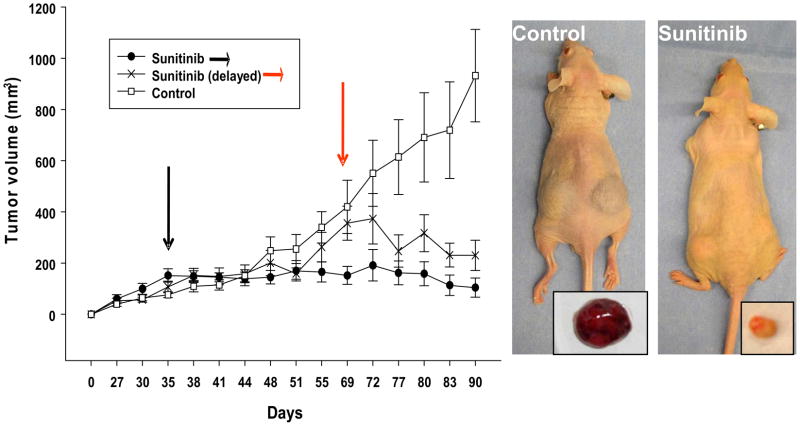
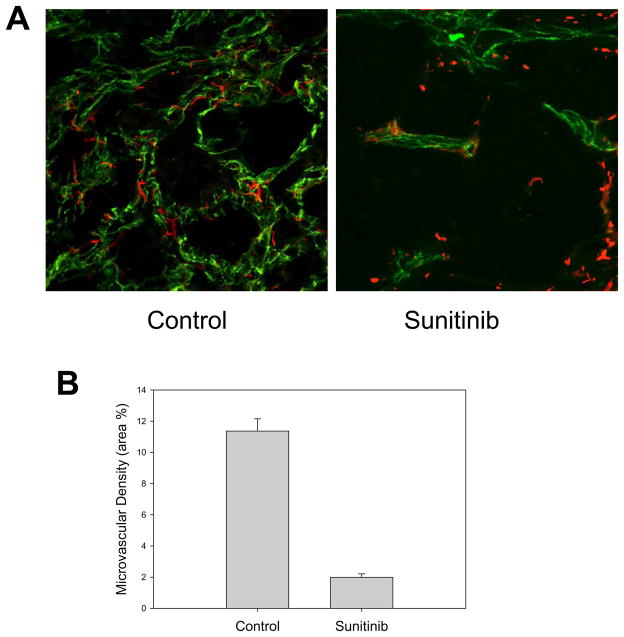
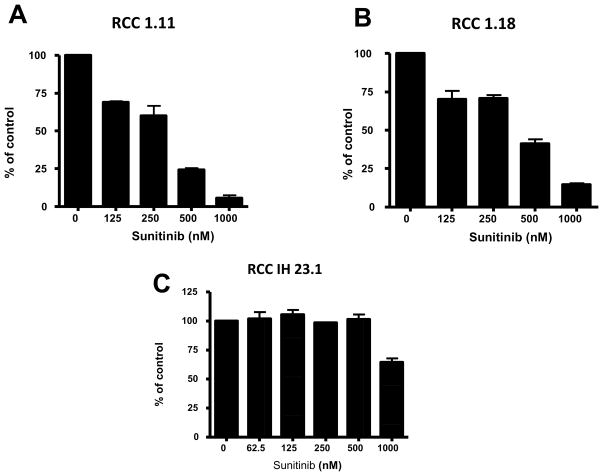
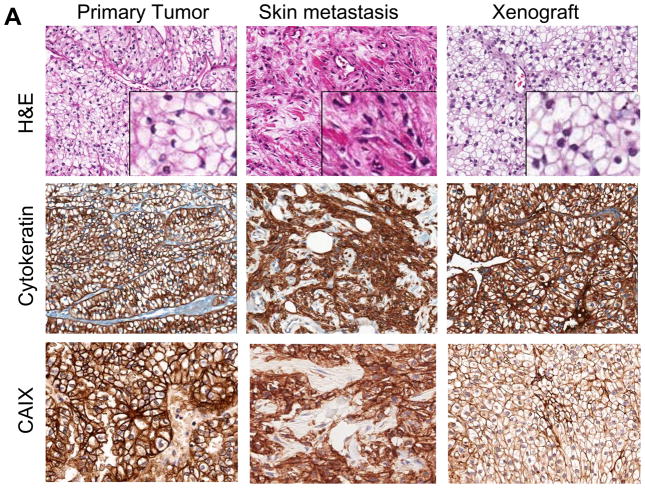
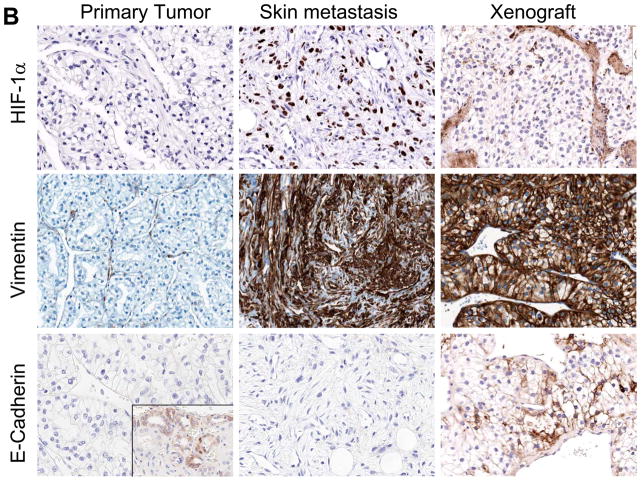
Tyrosine kinase inhibitors (TKI) targeting angiogenesis via inhibition of the vascular endothelial growth factor pathway have changed the medical management of metastatic renal cell carcinoma. Although treatment with TKIs has shown clinical benefit, these drugs will eventually fail patients. The potential mechanisms of resistance to TKIs are poorly understood. To address this question, we obtained an excisional biopsy of a skin metastasis from a patient with clear cell renal carcinoma who initially had a response to sunitinib and eventually progressed with therapy. Tumor pieces were grafted s.c. in athymic nude mice. Established xenografts were treated with sunitinib. Tumor size, microvascular density, and pericyte coverage were determined. Plasma as well as tissue levels for sunitinib were assessed. A tumor-derived cell line was established and assessed in vitro for potential direct antitumor effects of sunitinib. To our surprise, xenografts from the patient who progressed on sunitinib regained sensitivity to the drug. At a dose of 40 mg/kg, sunitinib caused regression of the subcutaneous tumors. Histology showed a marked reduction in microvascular density and pericyte dysfunction. More interestingly, histologic examination of the original skin metastasis revealed evidence of epithelial to mesenchymal transition, whereas the xenografts showed reversion to the clear cell phenotype. In vitro studies showed no inhibitory effect on tumor cell growth at pharmacologically relevant concentrations. In conclusion, the histologic examination in this xenograft study suggests that reversible epithelial to mesenchymal transition may be associated with acquired tumor resistance to TKIs in patients with clear cell renal carcinoma.
Figures
References
-
- Rini BI, Campbell SC, Escudier B. Renal cell carcinoma. Lancet. 2009;373(9669):1119–32. - PubMed
-
- Fabian MA, Biggs WH, 3rd, Treiber DK, Atteridge CE, Azimioara MD, Benedetti MG, et al. A small molecule-kinase interaction map for clinical kinase inhibitors. Nat Biotechnol. 2005;23(3):329–36. - PubMed
-
- Stein MN, Flaherty KT. CCR drug updates: Sorafenib and sunitinib in renal cell carcinoma. Clin Cancer Res. 2007;13(13):3765–70. - PubMed
-
- Motzer RJ, Michaelson MD, Redman BG, et al. Activity of SU11248, a multitargeted inhibitor of vascular endothelial growth factor receptor and platelet-derived growth factor receptor, in patients with metastatic renal cell carcinoma. J Clin Oncol. 2006;24(1):16–24. - PubMed
-
- Maxwell PH, Wiesener MS, Chang GW, et al. The tumour suppressor protein VHL targets hypoxia-inducible factors for oxygen-dependent proteolysis. Nature. 1999;399(6733):271–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
