

A molecular classifier for predicting future graft loss in late kidney transplant biopsies
- PMID: 20501945
- PMCID: PMC2877953
- DOI: 10.1172/JCI41789
A molecular classifier for predicting future graft loss in late kidney transplant biopsies
Abstract
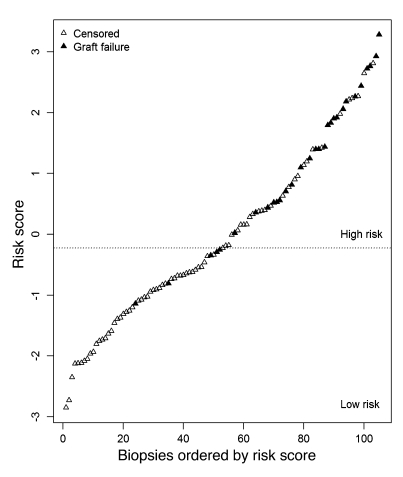
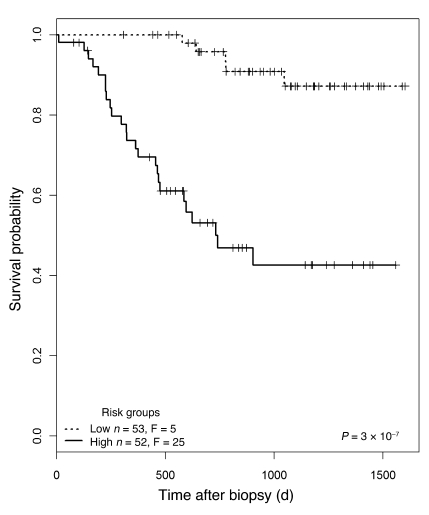
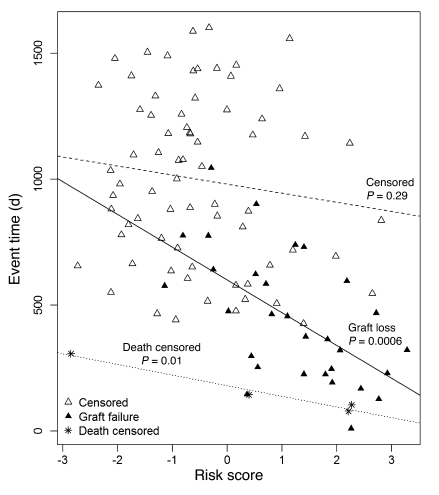
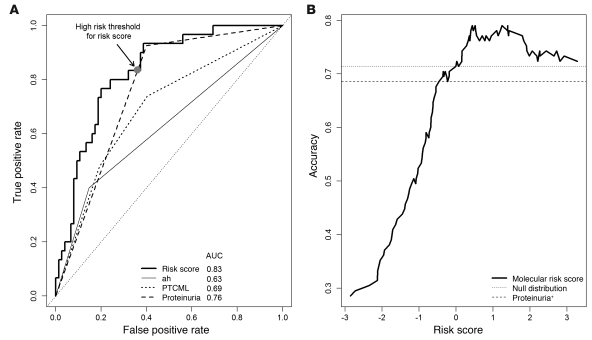
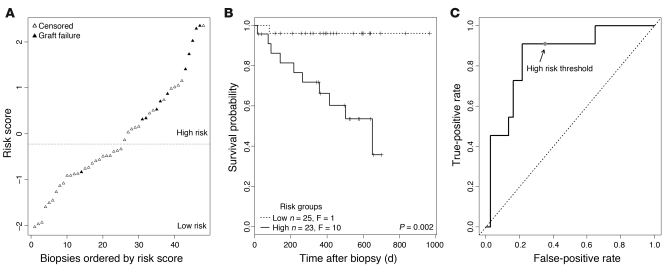
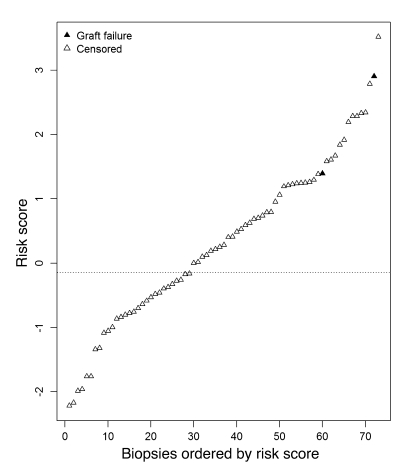
Kidney transplant recipients that develop signs of renal dysfunction or proteinuria one or more years after transplantation are at considerable risk for progression to renal failure. To assess the kidney at this time, a "for-cause" biopsy is performed, but this provides little indication as to which recipients will go on to organ failure. In an attempt to identify molecules that could provide this information, we used microarrays to analyze gene expression in 105 for-cause biopsies taken between 1 and 31 years after transplantation. Using supervised principal components analysis, we derived a molecular classifier to predict graft loss. The genes associated with graft failure were related to tissue injury, epithelial dedifferentiation, matrix remodeling, and TGF-beta effects and showed little overlap with rejection-associated genes. We assigned a prognostic molecular risk score to each patient, identifying those at high or low risk for graft loss. The molecular risk score was correlated with interstitial fibrosis, tubular atrophy, tubulitis, interstitial inflammation, proteinuria, and glomerular filtration rate. In multivariate analysis, molecular risk score, peritubular capillary basement membrane multilayering, arteriolar hyalinosis, and proteinuria were independent predictors of graft loss. In an independent validation set, the molecular risk score was the only predictor of graft loss. Thus, the molecular risk score reflects active injury and is superior to either scarring or function in predicting graft failure.
Figures
Comment in
-
Gazing into a crystal ball to predict kidney transplant outcome.J Clin Invest. 2010 Jun;120(6):1803-6. doi: 10.1172/JCI43286. Epub 2010 May 24. J Clin Invest. 2010. PMID: 20501950 Free PMC article.
References
-
- Colvin RB, et al. Evaluation of pathologic criteria for acute renal allograft rejection: reproducibility, sensitivity, and clinical correlation. J Am Soc Nephrol. 1997;8(12):1930–1941. - PubMed
-
- Agodoa L, et al. Assessment of structure and function in progressive renal disease. Kidney Int Suppl. 1997;63:S144–S150. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
