

Utilization and outcome of 'out-of-center hemodialysis' in the United States: a contemporary analysis
- PMID: 20502039
- PMCID: PMC2939990
- DOI: 10.1159/000314663
Utilization and outcome of 'out-of-center hemodialysis' in the United States: a contemporary analysis
Abstract
Background: There is increasing interest in the delivery of out-of-center hemodialysis (HD), particularly in the home setting, but little systematic information about its use and outcome in contemporary incident patients is available.
Patients and methods: Out-of-center HD was defined as HD delivered in a residential setting, mainly at home or in a long-term care facility (such as a nursing home) irrespective of the length and frequency of therapy. All-cause mortality was determined in an observational cohort study of 458,329 adult patients initiating dialysis in the United States with Medicare as a primary payer.
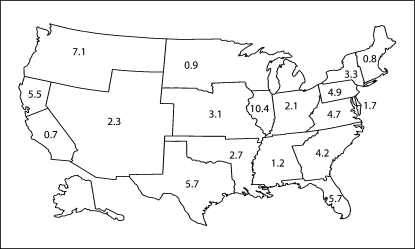
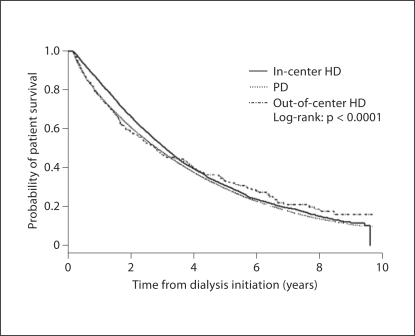
Results: Between 1995 and 2004, out-of-center HD was the initial modality in 1,641 (0.4%) of eligible participants, although there was significant geographic variation. Patients initiating out-of-center HD were younger, more likely to be nonwhite, had fewer comorbidities, a higher median income, and were more likely to be employed than patients initiating in-center HD or peritoneal dialysis (PD). In multivariate analysis, out-of-center HD patients had a higher overall risk of death compared to in-center HD or PD patients (HR = 1.10, 95% CI 1.04, 1.17), although the relative risk of death was lower in younger and healthier patients (HR = 0.78; 95% CI 0.61, 1.00).
Conclusion: Out-of-center HD is not associated with a survival advantage among unselected patients initiating dialysis in the United States. These results call for better characterization of out-of-center HD in national registries, primarily to effectively compare the use, outcomes and potential benefits of home HD to standard therapies.
Figures
References
-
- Shaldon S. Origin of home haemodialysis. Nephrol Dial Transplant. 2006;21:3610–3611. - PubMed
-
- Blagg CR. Home haemodialysis: ‘home, home, sweet, sweet home!’. Nephrology. 2005;10:206–214. - PubMed
-
- Saner E, Nitsch D, Descoeudres C, Frey FJ, Uehlinger DE. Outcome of home haemodialysis patients: a case-cohort study. Nephrol Dial Transplant. 2005;20:604–610. - PubMed
-
- Nesrallah GE, Moist LM, Awaraji C, Lindsay RM. An international registry to compare quotidian dialysis regimens with conventional thrice-weekly hemodialysis: why, how and potential pitfalls. Semin Dial. 2004;17:131–135. - PubMed
-
- Kjellstrand CM, Buoncristiani U, Ting G, Traeger J, Piccoli GB, Sibai-Galland R, Young BA, Blagg CR. Short daily haemodialysis: survival in 415 patients treated for 1006 patient-years. Nephrol Dial Transplant. 2008;23:3283–3289. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
