

Clinicopathological features and prognosis assessment of extranodal follicular dendritic cell sarcoma
- PMID: 20503450
- PMCID: PMC2877180
- DOI: 10.3748/wjg.v16.i20.2504
Clinicopathological features and prognosis assessment of extranodal follicular dendritic cell sarcoma
Abstract
Aim: To establish a model for prognosis assessment of extranodal follicular dendritic cell (FDC) sarcoma.
Methods: Nine lesions were examined by routine and molecular approaches. Clinicopathological factors from the new cases and 97 reported cases were analyzed for their prognostic values.
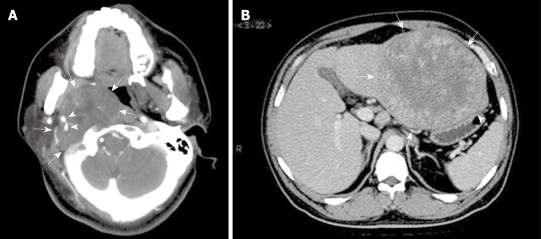
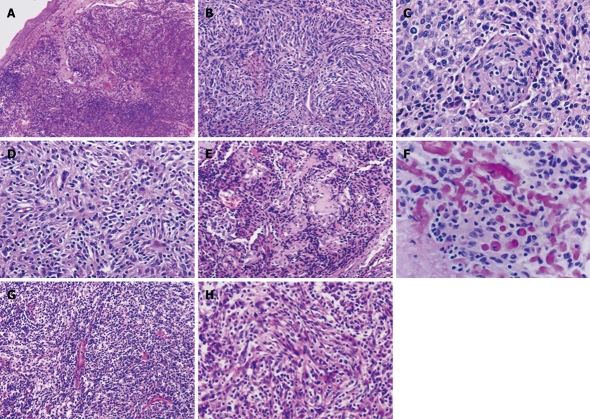
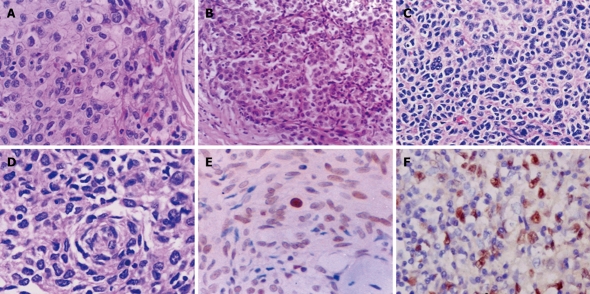
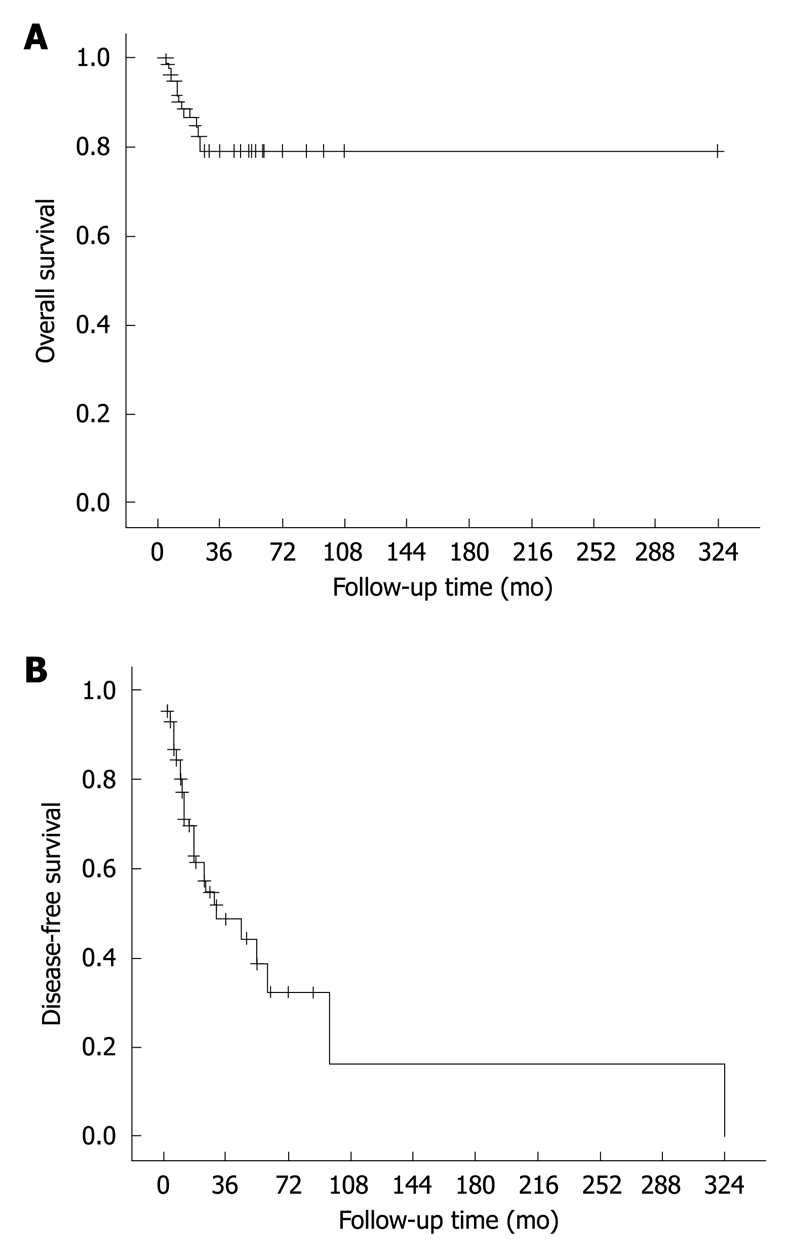
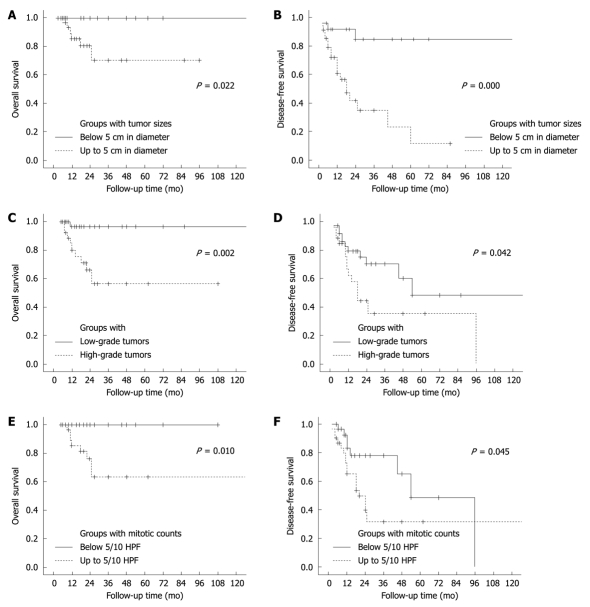
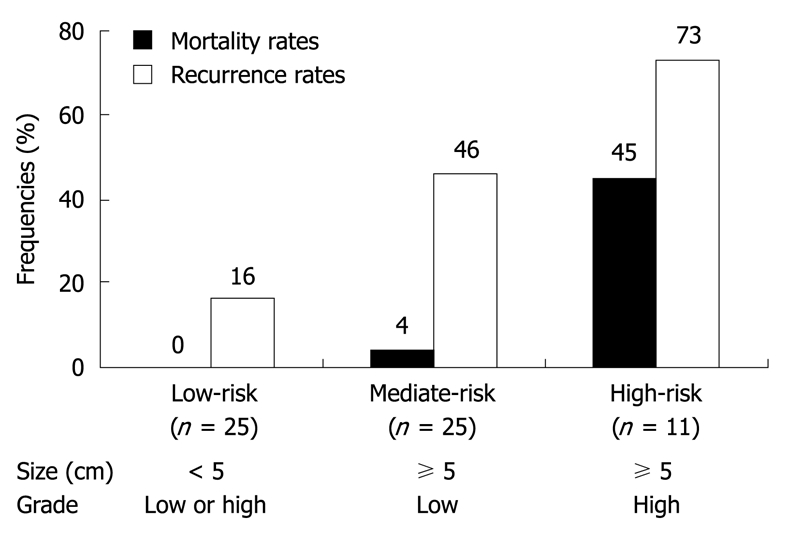
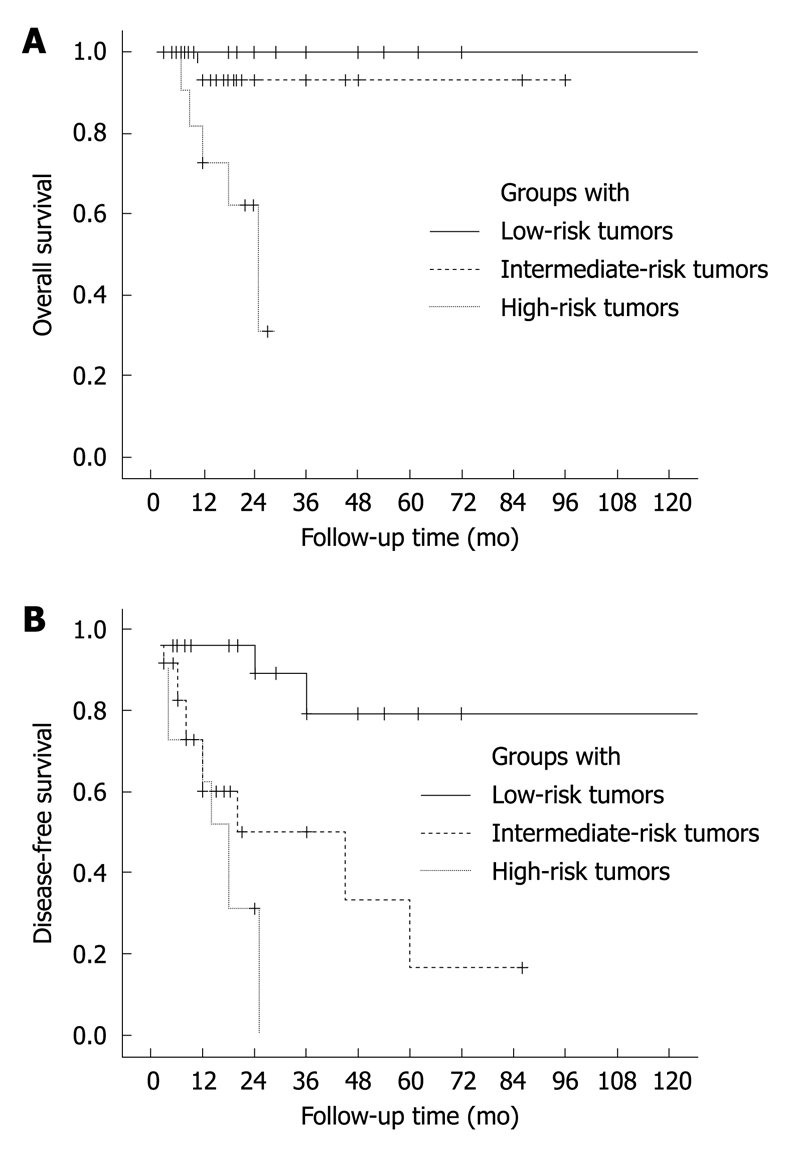
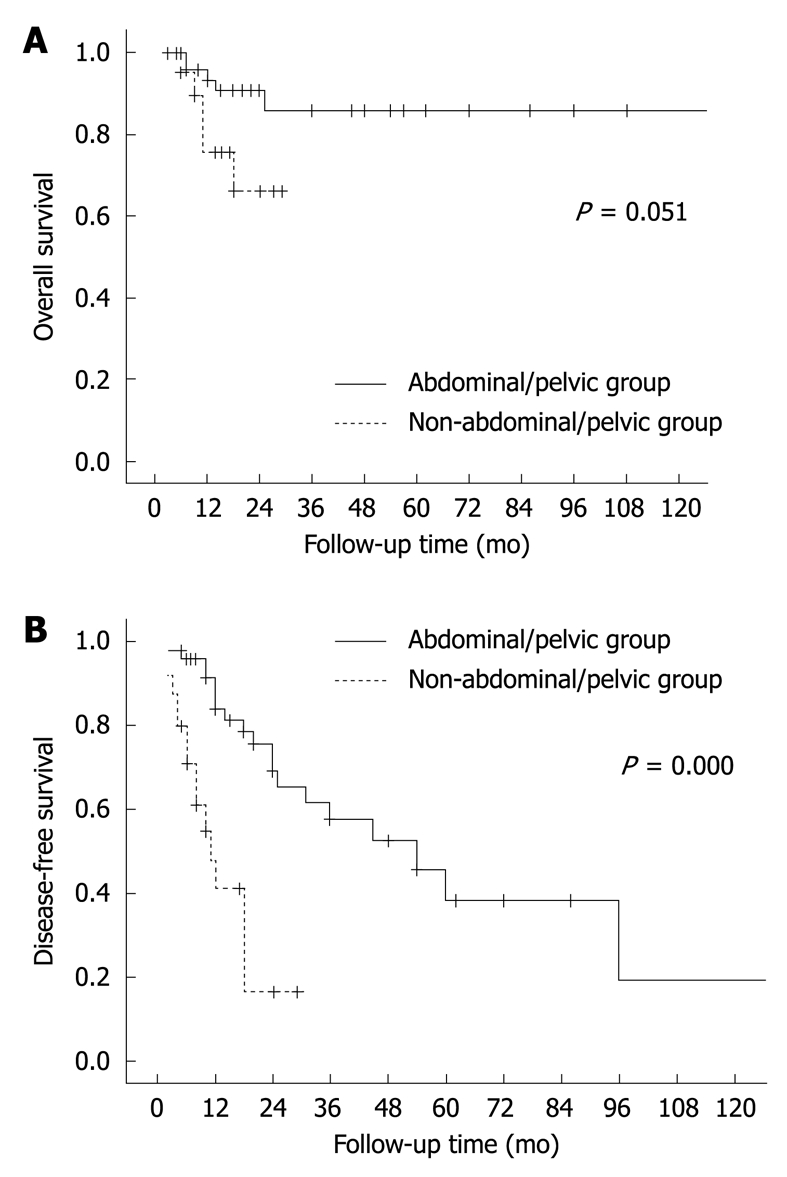
Results: The current lesions were found in five male and four female patients, located mainly in the head and neck area and averaging 7.2 cm in size. Six patients had recurrence or metastasis and three remained free of disease. The 106 patients (male/female ratio, 1.1:1) were aged from 9 to 82 years (median, 44 years). The tumor sizes ranged from 1.5 to 21 cm (mean, 7.4 cm). Abdominal/pelvic region was affected most frequently (43%). Surgical resection was performed in 100 patients, followed by radiation and/or chemotherapy in 35 of them. Follow-up data were available in 91 cases, covering a period of 3-324 mo (mean, 27 mo; median, 19 mo). Of the informative cases, 38 (42%) had recurrence or metastasis, and 12 (13%) died of the disease. These tumors were classified histologically into low- and high-grade lesions. A size > or = 5 cm (P = 0.003), high-grade histology (P = 0.046) and a mitotic count > or = 5/10 HPF (P = 0.013) were associated with tumor recurrence. The lesions were defined as low-, intermediate- and high-risk tumors, and their recurrence rates were 16%, 46% and 73%, and their mortality rates 0%, 4% and 45%, respectively.
Conclusion: Extranodal FDC tumors behave like soft tissue sarcomas. Their clinical outcomes are variable and can be evaluated according to their sizes and grades.
Figures
References
-
- Pileri SA, Grogan TM, Harris NL, Banks P, Campo E, Chan JK, Favera RD, Delsol G, De Wolf-Peeters C, Falini B, et al. Tumours of histiocytes and accessory dendritic cells: an immunohistochemical approach to classification from the International Lymphoma Study Group based on 61 cases. Histopathology. 2002;41:1–29. - PubMed
-
- Chan JK, Fletcher CD, Nayler SJ, Cooper K. Follicular dendritic cell sarcoma. Clinicopathologic analysis of 17 cases suggesting a malignant potential higher than currently recognized. Cancer. 1997;79:294–313. - PubMed
-
- Cheuk W, Chan JK, Shek TW, Chang JH, Tsou MH, Yuen NW, Ng WF, Chan AC, Prat J. Inflammatory pseudotumor-like follicular dendritic cell tumor: a distinctive low-grade malignant intra-abdominal neoplasm with consistent Epstein-Barr virus association. Am J Surg Pathol. 2001;25:721–731. - PubMed
-
- Chen TC, Kuo TT, Ng KF. Follicular dendritic cell tumor of the liver: a clinicopathologic and Epstein-Barr virus study of two cases. Mod Pathol. 2001;14:354–360. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
