

doi: 10.1093/eurheartj/ehq152.
Epub 2010 May 26.
Pulmonary arterial hypertension: from the kingdom of the near-dead to multiple clinical trial meta-analyses
Affiliations
- PMID: 20504865
- PMCID: PMC2930983
- DOI: 10.1093/eurheartj/ehq152
Item in Clipboard
Pulmonary arterial hypertension: from the kingdom of the near-dead to multiple clinical trial meta-analyses
Eur Heart J.
2010 Sep.
No abstract available
Figures
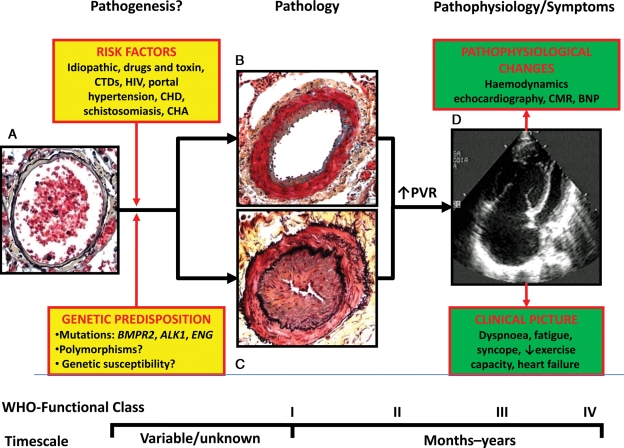
Schematic representation of pathogenesis, pathology, pathophysiology, and symptoms in pulmonary arterial hypertension. (A) Normal small distal pulmonary artery: the thin wall is constituted by a single elastic lamina and a thin layer of smooth muscle cells; a large lumen with red blood cells is also shown. (B) Distal pulmonary artery in pulmonary arterial hypertension: increased thickness of the media due to hypertrophy and hyperplasia of smooth muscle cells and moderate lumen reduction are present. This picture may represent an initial phase of the disease and/or the prevalent changes in patients responding to vasoreactivity tests. (C) Distal pulmonary artery in pulmonary arterial hypertension: increased thickness of the media and also of the intima due to proliferation/migration of myofibroblasts and fibrosis are present. Severe lumen reduction is also shown. This picture may represent an advanced phase of the disease and/or the prevalent changes in patients not responding to vasoreactivity tests. (D) Echocardiographic four-chamber view in pulmonary arterial hypertension: Severe dilatation of the right atrium and ventricle and reduction in size of the left ventricle are shown. ALK1, activin-like kinase-type 1 gene; BNP, brain natriuretic peptide; BMPR2, bone morphogenetic protein receptor type 2 gene; CHA, chronic haemolytic anaemia; CHD, congenital heart disease; CTD, connective tissue diseases; ENG, endoglin gene; HIV, human immunodeficiency virus; CMR, cardiac magnetic resonance; PAH, pulmonary arterial hypertension; PVR, pulmonary vascular resistance; WHO, world health organization. The pathological pictures are a courtesy of Dr Carol Farver, Cleveland Clinic.
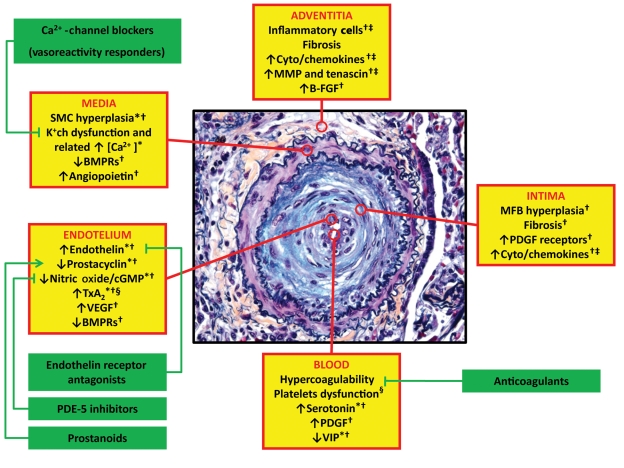
Obstructive remodelling of a small pulmonary artery in pulmonary arterial hypertension (increased thickness of the three vessel layers and severe lumen reduction are shown) and ongoing pathobiological processes in the different layers of the vessel wall (yellow boxes) and in the blood. Asterisks indicate the potential processes involved. Corrective interactions of the related approved therapeutic interventions are also reported (green boxes). *Vasoconstriction; †Proliferation/migration; ‡Inflammation; §Thrombosis. B-FGF, basic fibroblast growth factor; BMPR, bone morphogenetic protein receptor; [Ca2+], intracellular calcium concentration; K+ch, membrane potassium channels; SMC, smooth muscle cells; MFB, myofibroblasts; MMP, matrix metalloproteases; PDE-5, phosphodiesterase type 5; PDGF, platelet-derived growth factor; TxA2, tromboxane A2; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal peptide. The pathological picture is a courtesy of Dr Carol Farver, Cleveland Clinic.
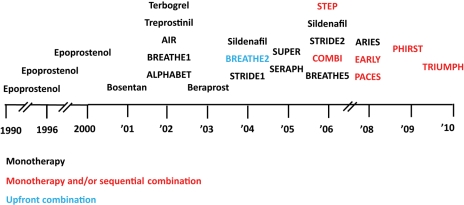
Time-course of 25 published randomized controlled studies (identified by acronyms, if any, or drug and year of publication) in pulmonary arterial hypertension as of May 2010. Colour code identifies the design of the study: monotherapy (black): investigational drug vs. placebo in patients naive for pulmonary arterial hypertension approved drugs. Monotherapy and/or sequential combination (red): investigational drug vs. placebo in patients either naive for, or treated with pulmonary arterial hypertension approved drugs. Upfront combination (light blue): single drug vs. combination of two drugs in patients naive for pulmonary arterial hypertension approved drugs.
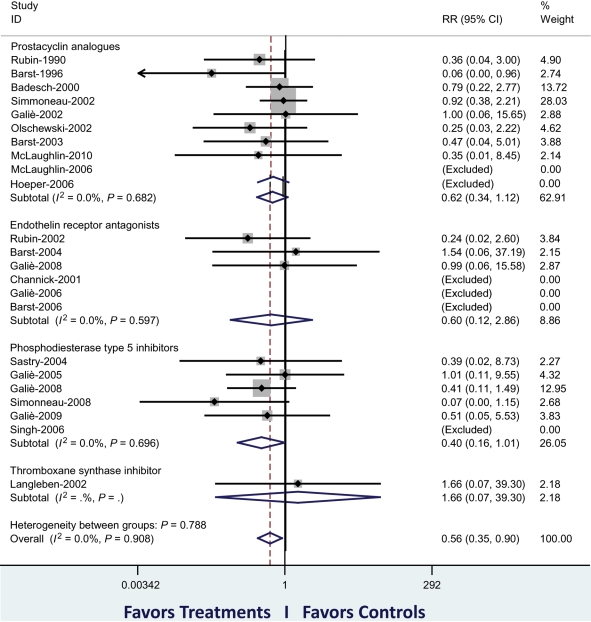
Meta-analysis of published randomized controlled studies (identified by first author and year of publication) in pulmonary arterial hypertension as of May 2010. The primary analysis has included 3780 patients of 23 trials. The figure shows the cumulative RR estimate of death in active treatment groups when compared with control groups stratified according to treatment class (inverse variance method). Studies with no events in both groups were excluded. An overall reduction of mortality of 44% (P = 0.016) is shown. The sensitivity analysis, including two additional studies (59 patients) in which two treatment strategies were compared, confirmed a reduction in mortality of 39% (P = 0.041). The subgroup analysis of the three classes of approved drugs achieved a similar favourable reduction in mortality, although no statistical significance was achieved individually. RR, relative risk. Modified from Galiè et al.12
References
-
- Galiè N, Hoeper M, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Klepetko W, Joendeau G, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G. Guidelines on diagnosis and treatment of pulmonary hypertension: the Task Force on Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology and of the European Respiratory Society. Eur Heart J. 2009;30:2493–2537. - PubMed
-
- Peacock AJ, Murphy NF, McMurray JJV, Caballero L, Stewart S. An epidemiological study of pulmonary arterial hypertension. Eur Respir J. 2007;30:104–109. doi:10.1183/09031936.00092306. - DOI - PubMed
-
- Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaici A, Weitzenblum E, Cordier JF, Chabot F, Dromer C, Pison C, Reynaud-Gaubert M, Haloun A, Laurent M, Hachulla E, Simonneau G. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173:1023–1030. doi:10.1164/rccm.200510-1668OC. - DOI - PubMed
-
- Pietra GG, Capron F, Stewart S, Leone O, Humbert M, Robbins IM, Reid LM, Tuder RM. Pathologic assessment of vasculopathies in pulmonary hypertension. J Am Coll Cardiol. 2004;43(Suppl. 12):S25–S32. doi:10.1016/j.jacc.2004.02.033. - DOI - PubMed
-
- Tuder RM, Abman SH, Braun T, Capron F, Stevens T, Thistlethwaite PA, Haworth S. Pulmonary circulation: development and pathology. J Am Coll Cardiol. 2009;54:S3–S9. doi:10.1016/j.jacc.2009.04.009. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
