

Stenting versus endarterectomy for treatment of carotid-artery stenosis
- PMID: 20505173
- PMCID: PMC2932446
- DOI: 10.1056/NEJMoa0912321
Stenting versus endarterectomy for treatment of carotid-artery stenosis
Erratum in
- N Engl J Med. 2010 Jul 29;363(5):498
- N Engl J Med. 2010 Jul 8;363(2):198
Abstract
Background: Carotid-artery stenting and carotid endarterectomy are both options for treating carotid-artery stenosis, an important cause of stroke.
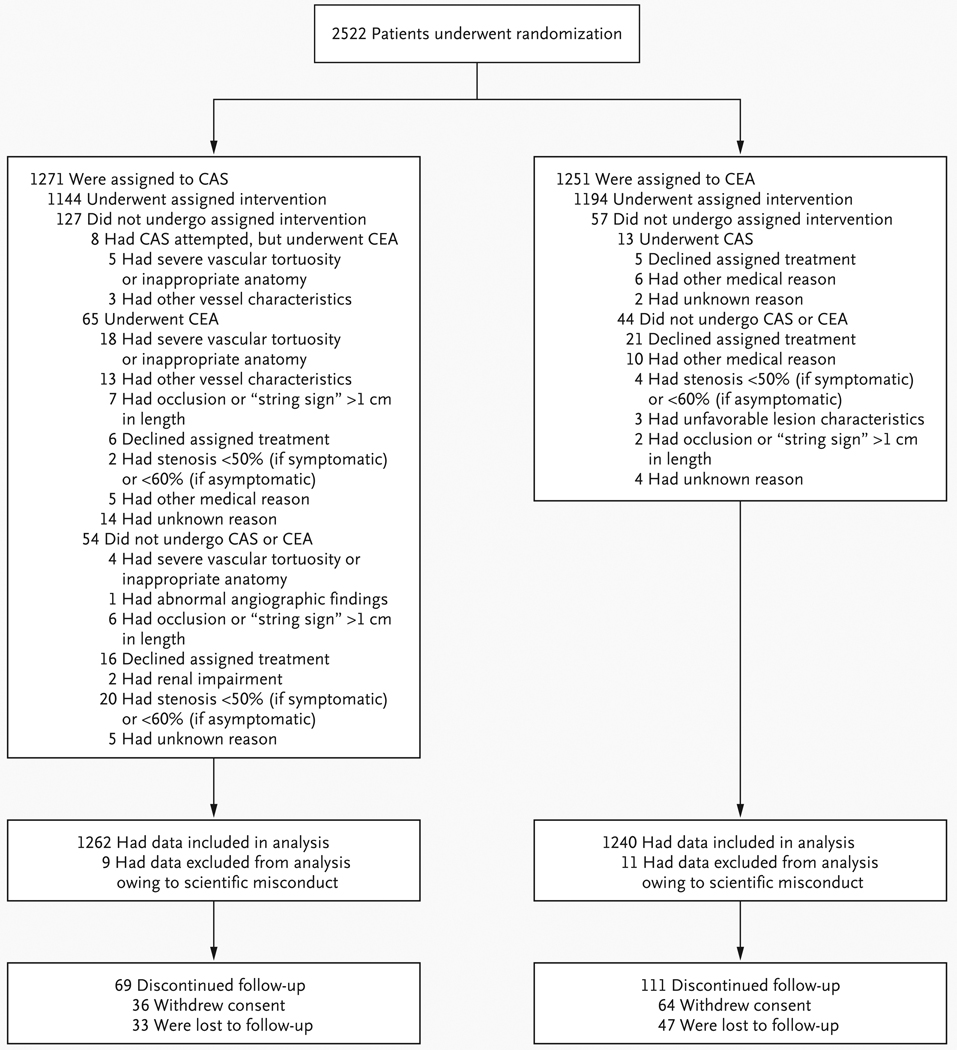
Methods: We randomly assigned patients with symptomatic or asymptomatic carotid stenosis to undergo carotid-artery stenting or carotid endarterectomy. The primary composite end point was stroke, myocardial infarction, or death from any cause during the periprocedural period or any ipsilateral stroke within 4 years after randomization.
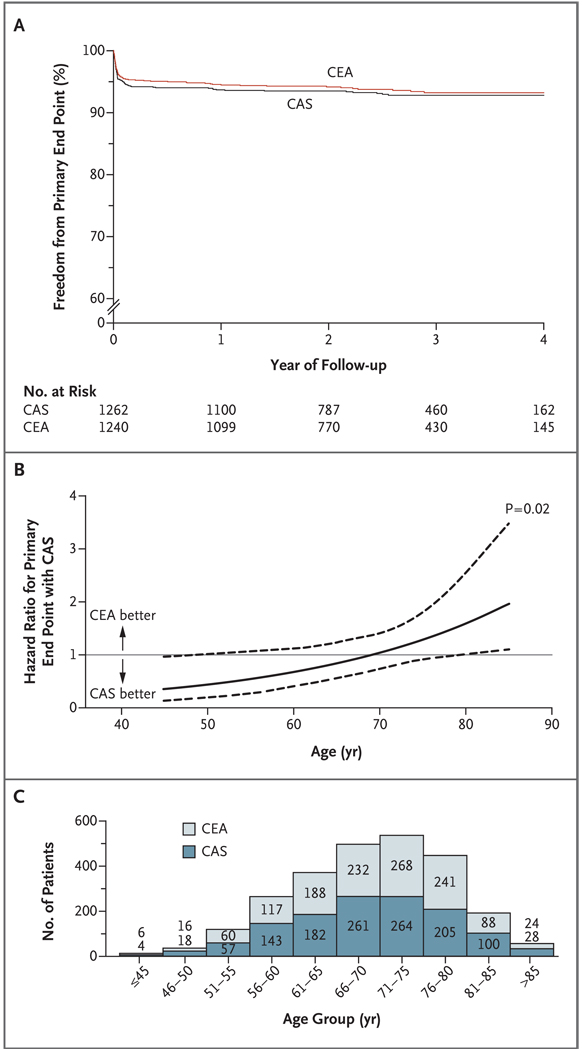
Results: For 2502 patients over a median follow-up period of 2.5 years, there was no significant difference in the estimated 4-year rates of the primary end point between the stenting group and the endarterectomy group (7.2% and 6.8%, respectively; hazard ratio with stenting, 1.11; 95% confidence interval, 0.81 to 1.51; P=0.51). There was no differential treatment effect with regard to the primary end point according to symptomatic status (P=0.84) or sex (P=0.34). The 4-year rate of stroke or death was 6.4% with stenting and 4.7% with endarterectomy (hazard ratio, 1.50; P=0.03); the rates among symptomatic patients were 8.0% and 6.4% (hazard ratio, 1.37; P=0.14), and the rates among asymptomatic patients were 4.5% and 2.7% (hazard ratio, 1.86; P=0.07), respectively. Periprocedural rates of individual components of the end points differed between the stenting group and the endarterectomy group: for death (0.7% vs. 0.3%, P=0.18), for stroke (4.1% vs. 2.3%, P=0.01), and for myocardial infarction (1.1% vs. 2.3%, P=0.03). After this period, the incidences of ipsilateral stroke with stenting and with endarterectomy were similarly low (2.0% and 2.4%, respectively; P=0.85).
Conclusions: Among patients with symptomatic or asymptomatic carotid stenosis, the risk of the composite primary outcome of stroke, myocardial infarction, or death did not differ significantly in the group undergoing carotid-artery stenting and the group undergoing carotid endarterectomy. During the periprocedural period, there was a higher risk of stroke with stenting and a higher risk of myocardial infarction with endarterectomy. (ClinicalTrials.gov number, NCT00004732.)
2010 Massachusetts Medical Society
Figures
Comment in
-
Carotid-artery stenting in stroke prevention.N Engl J Med. 2010 Jul 1;363(1):80-2. doi: 10.1056/NEJMe1005220. Epub 2010 May 26. N Engl J Med. 2010. PMID: 20505174 No abstract available.
-
Stroke: high rate of occult atrial fibrillation, effects of insulin on growth of infarction and stenting versus endarterectomy for treatment of carotid-artery stenosis.J Neurol. 2010 Jul;257(7):1221-3. doi: 10.1007/s00415-010-5628-y. J Neurol. 2010. PMID: 20559840 No abstract available.
-
[Endarterectomy compared to stenting in treatment of carotid artery stenosis - treatment outcome CREST].Kardiol Pol. 2010 Sep;68(9):1083-5. Kardiol Pol. 2010. PMID: 20859913 Polish. No abstract available.
-
Is endovascular stent therapy or endarterectomy more effective for the treatment of symptomatic and asymptomatic carotid stenosis?Curr Cardiol Rep. 2011 Feb;13(1):1-2. doi: 10.1007/s11886-010-0145-2. Curr Cardiol Rep. 2011. PMID: 20882370 No abstract available.
-
Carotid stenting or surgical carotid endarterectomy to prevent strokes?Expert Rev Cardiovasc Ther. 2010 Oct;8(10):1379-81. doi: 10.1586/erc.10.94. Expert Rev Cardiovasc Ther. 2010. PMID: 20936923
-
Stenting versus endarterectomy for carotid-artery stenosis.N Engl J Med. 2010 Oct 28;363(18):1766; author reply 1768. doi: 10.1056/NEJMc1009626. N Engl J Med. 2010. PMID: 20979480 No abstract available.
-
Stenting versus endarterectomy for carotid-artery stenosis.N Engl J Med. 2010 Oct 28;363(18):1766-7; author reply 1768. doi: 10.1056/NEJMc1009626. N Engl J Med. 2010. PMID: 21038510 No abstract available.
-
Stenting versus endarterectomy for carotid-artery stenosis.N Engl J Med. 2010 Oct 28;363(18):1767; author reply 1768. doi: 10.1056/NEJMc1009626. N Engl J Med. 2010. PMID: 21038511 No abstract available.
-
Stenting versus endarterectomy for carotid-artery stenosis.N Engl J Med. 2010 Oct 28;363(18):1767-8; author reply 1768. doi: 10.1056/NEJMc1009626. N Engl J Med. 2010. PMID: 21038512 No abstract available.
-
ACP Journal Club. Stenting and endarterectomy for carotid artery stenosis did not differ for a composite of stroke, MI, or death.Ann Intern Med. 2010 Nov 16;153(10):JC5-12. doi: 10.7326/0003-4819-153-10-201011160-02012. Ann Intern Med. 2010. PMID: 21079207 No abstract available.
References
-
- Petty GW, Brown RD, Jr, Whisnant JP, Sicks JD, O’Fallon WM, Wiebers DO. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke. 1999;30:2513–2516. - PubMed
-
- Goldstein LB, Adams R, Alberts MJ, et al. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group: The American Academy of Neurology affirms the value of this guideline. Stroke. 2006;37:1583–1633. [Erratum, Stroke 2007;38:207.] - PubMed
-
- Ederle J, Featherstone RL, Brown MM. Percutaneous transluminal angioplasty and stenting for carotid artery stenosis. Cochrane Database Syst Rev. 2007;4:CD000515. - PubMed
-
- Yadav JS, Wholey MH, Kuntz RE, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351:1493–1501. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical