

Apoptosis during CABG surgery with the use of cardiopulmonary bypass is prominent in ventricular but not in atrial myocardium
- PMID: 20505796
- PMCID: PMC2871743
- DOI: 10.1007/BF03091769
Apoptosis during CABG surgery with the use of cardiopulmonary bypass is prominent in ventricular but not in atrial myocardium
Abstract
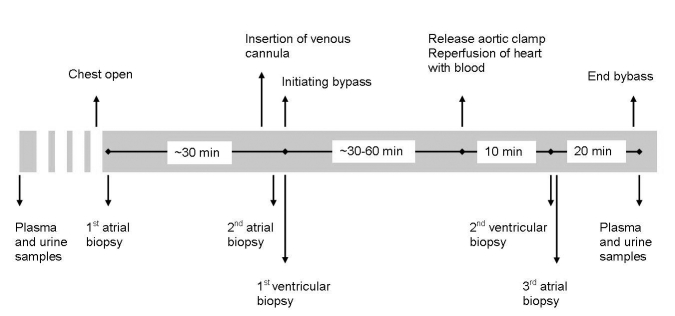
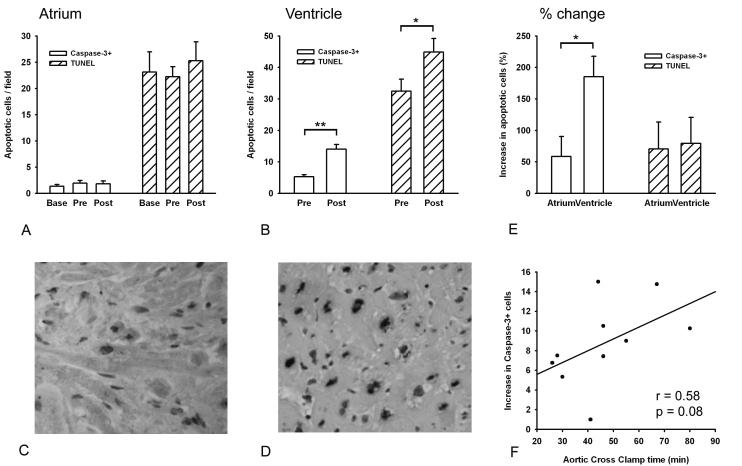
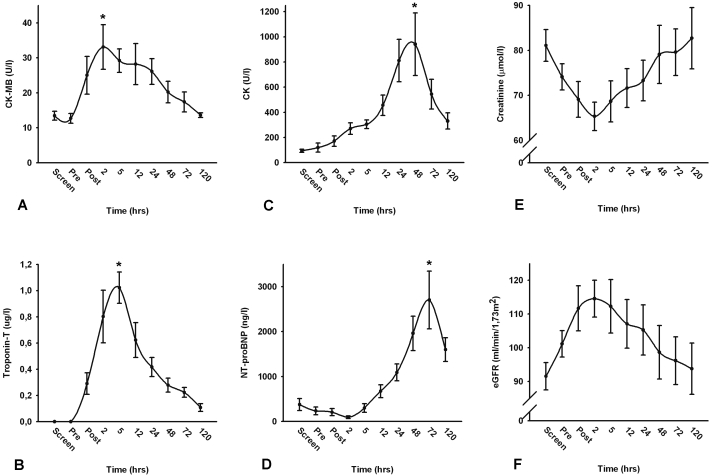
Objectives. We aimed to compare the rate of apoptosis after cardiopulmonary bypass (CPB) and cardioplegic arrest during coronary artery bypass grafting (CABG) surgery between atrial and ventricular tissue.Methods. During CABG surgery with CPB and cardioplegic arrest, sequential biopsies were taken from the right atrial appendage and left ventricular anterior wall before CPB and after aortic cross clamp release. Change in number of apoptotic cells and biochemical markers of myocardial ischaemia and renal dysfunction were assessed.Results. CPB was associated with a transient small, but significant increase in CK (1091+/-374%), CK-MB (128+/-38%), troponin-T (102+/-13%) and NT-proBNP (1308+/-372%) levels (all: p<0.05). A higher number of apoptotic cells as assessed by caspase-3 staining was found in the ventricular biopsies taken after aortic cross clamp release compared with the biopsies taken before CPB (5.3+/-0.6 vs. 14.0+/-1.5 cells/microscopic field, p<0.01). The number of apoptotic cells in the atrial appendage was not altered during CPB. Correlation between the duration of aortic cross clamp time and the change in caspase-3 positive cells in the left ventricular wall was of borderline significance (r of 0.58, p=0.08). Similar results were obtained from TUNEL staining for apoptosis.Conclusion. CABG surgery with CPB and cardioplegic arrest is associated with an elevated rate of apoptosis in ventricular but not in atrial myocardial tissue. Ventricular tissue may be more sensitive to detect changes than atrial tissue, and may be more useful to investigate the protective effects of therapeutic intervention. (Neth Heart J 2010;18:236-42.).
Keywords: Apoptosis; Coronary Artery Bypass; Heart Arrest; Heart Atria; Heart vetricules; Reperfusion Injury.
Figures
References
-
- Alexiou K, Kappert U, Staroske A, Joskowiak D, Wilbring M, Matschke K, et al. Coronary surgery for acute coronary syndrome: which determinants of outcome remain? Clin Res Cardiol. 2008;97:601-8. - PubMed
-
- Becker LB. New concepts in reactive oxygen species and cardiovascular reperfusion physiology. Cardiovasc Res. 2004;61:461-70. - PubMed
-
- Taniyama Y, Griendling KK. Reactive oxygen species in the vasculature: molecular and cellular mechanisms. Hypertension. 2003;42:1075-81. - PubMed
-
- Sugden PH, Clerk A. Oxidative stress and growth-regulating intracellular signaling pathways in cardiac myocytes. Antioxid Redox Signal. 2006;8:2111-24. - PubMed
-
- Sabbah HN, Sharov VG, Goldstein S. Cell death, tissue hypoxia and the progression of heart failure. Heart Fail Rev. 2000;5:131-8. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous